
During the COVID-19 pandemic, global health services have endeavoured to limit transmission and prioritise access to urgent care. This presented a challenge to the ongoing management of long-term conditions, including lymphoedema care. Damage to the lymphatic system can cause chronic swelling and a myriad of problems for patients that affect their health, wellbeing and quality of life (Greene and Meskell, 2017; Todd, 2017; Mercier et al, 2019; Thomas et al, 2020).
In addition to patient stories, lymphoedema therapists typically rely on sensory data (visual and tactile information) to assess lymphoedema and plan care. However, the COVID-19 pandemic curtailed face-to-face appointments and led to access being rationed according to urgency of need. In response, virtual lymphoedema services were implemented; however, the impact on access (delayed appointments and referrals) and lymphoedema management (risk of deterioration as well as postponed intensive treatments) was unclear.
To protect patient care and foster resilience in staff and services the impact of new ways or working needs to be understood.
Understanding lymphoedema care during the COVID-19 pandemic
Initial scoping of staff perceptions regarding the impact of the pandemic on services, patients and roles as well as the acceptability of study method shaped the study. Four scoping questions were developed by both authors (Box 1).
Scoping data were collected via email from Lymphoedema Network Wales clinical lymphoedema leads in each of the seven NHS Wales health boards plus national team members over a 2-week period in April 2020. Responses were reviewed by both authors.
Aim
This evaluation aimed to understand the experiences of clinical and non-clinical lymphoedema staff during the COVID-19 pandemic using a cross-sectional online survey.
Method
Study design
Based on the initial scoping exercise, an online staff survey was created covering:
There was a free-text option for impromptu feedback. The response format included open and closed questions, multiple choice and a five-point Likert scale of agreement. Respondent demographic data were not collected.
Participants
The staff survey was shared with all contacts within the Lymphoedema Network Wales database (n=141). Of these, 96 were eligible to participate as clinical and non-clinical lymphoedema staff in Wales.
Data collection
The anonymous survey was hosted at Online Surveys for 3 weeks in June 2020 and was available in English and Welsh. The survey hyperlink was shared using email (n=96), with weekly email reminders of the deadline for completion. All staff were thanked for their hard work during the COVID-19 pandemic and reminded that participation was optional.
Analysis
Survey data were explored descriptively and managed using Microsoft Excel. Questions rated using a five-point Likert scale of agreement were weighted: strongly disagree -2; somewhat disagree -1, neither agree nor disagree 0; somewhat agree 1; and strongly agree 2. Free-text questions were analysed using thematic analysis.
Ethical considerations
Swansea Bay University Health Board undertook a research, ethical and governance review (15 May 2020), which confirmed this survey was a service evaluation.
Findings
From the eligible respondents (clinical and non-clinical substantive post in lymphoedema services), the response rate was 71% (68/96). Clinical and non-clinical respondents are reported together to preserve anonymity.
Respondents
Working in new locations
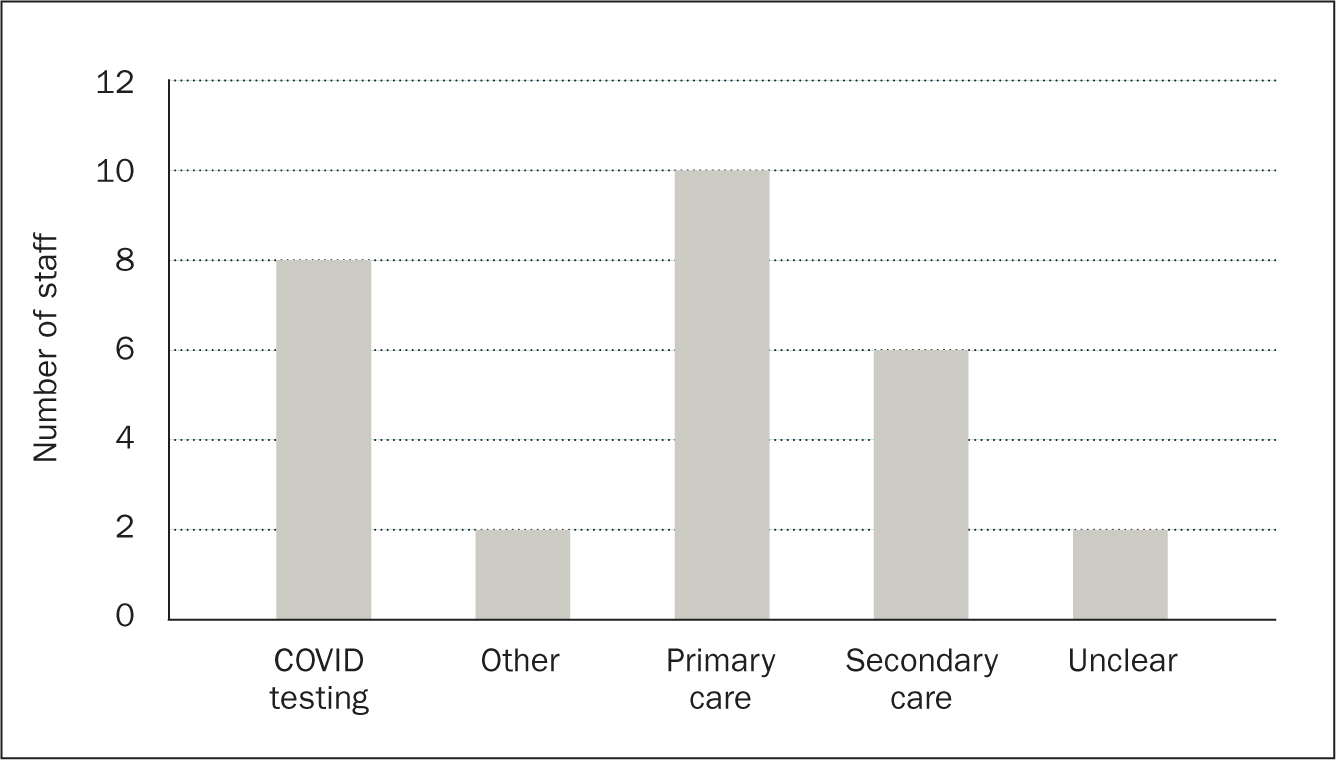
Fewer than half of lymphoedema staff were redeployed (41% 28/68) to other NHS sectors (Figure 1); 18 of them also supported lymphoedema services part time.
A similar proportion (40% 27/68) worked from home some or all of the time. Seven staff worked from home all the time. For those working in a new location (home or elsewhere; n=46), challenges with IT provision and support were reported (connectivity: 7/33; equipment: 12/37; and access to documents/databases: 11/35).
By the time the survey closed, some problems had been resolved; 30% of staff (10/33; weighted average 0.02) still did not have everything required to work from home, while 48% (16/33) did.
Preparation, training and experience of being redeployed
Most respondents felt adequately prepared (82% 23/28) and supported by staff in their new area (89% 25/28) and in the lymphoedema team (100%). Preparation for new roles included training and shadowing staff; some respondents had recent experience in that area. However, for some, the training was insufficient or they felt expected to learn on the job:
‘Learn as you go style … as the system/role changed weekly and now daily to cope with the workload and government guidelines for testing.’
‘I was given a list of patients my first day, no training given. However, I was previously a district nurse, so I expect they thought I would hit the ground running.’
Caring and supportive staff who pulled together were frequently cited to explain the positive experiences during difficult times:
‘[They were] extremely understanding … all in the same boat.’
‘When we were due to have our first COVID-19 positive patient, the senior sister stayed on to talk to us all before we began our shift. We all appreciated that.’
For the roles requiring personal protective equipment (PPE), overall PPE provision was adequate (18/22). However, for some respondents, inadequate PPE caused significant distress and for one explained the lack of support received during their deployment:
‘At one point, I was told to wash my face mask in the washing machine. Visors were acquired for the team but not for me.’
‘After I stood my ground on PPE I felt I was shunned.’
Reflecting on time spent in new areas, half the staff (14/28) identified new learning opportunities that could be shared with lymphoedema services covering virtual working and documentation:
‘Virtual assessments establish if face-to-face contact is needed.’
‘Remote working practices could free up more appointments for new or urgent patients. Leaflets being sent out to patients before their visit could encourage more patient empowerment’
‘Notes could be typed, which was more efficient, and information/referrals could be accessed more easily.’
Similarly, more than half of staff deployed identified how lymphoedema services could share their learning with other NHS sectors (15/28), focusing on knowledge of lymphoedema and its management:
‘[They have] very little understanding of lymphoedema and the consequences of it.’
‘[They] do not have the confidence to place patients in compression … [They] need education in the identification of mild to moderate oedema and when/how to refer these patients in order to prevent further deterioration.’
‘Basic lymphoedema management … more education on the wards in terms of basic lymphoedema management such the importance of the patient wearing their garments, how to don/doff garments, skin care and the importance of elevating legs during a hospital stay.’
All staff experiences during COVID-19
Working during the COVID-19 pandemic
Staff views of working during the COVID-19 pandemic are summarised (Table 1). Staff missed team working and, in particular, face-to-face contact. New skills were acquired and many viewed the opportunity to work differently positively. Interestingly, more than one quarter indicted that the chance to work in another area had made them consider changing their job. On the whole, staff did not travel more and used the opportunity for housekeeping and working effectively. Accordingly, more than half the workforce were busier than normal and fewer than half achieved a better home-work life balance.
| Survey item | Weighted average strength of agreement (n) |
|---|---|
| Responses sorted by strength of agreement and disagreement. Strong differences are in bold and moderate differences in italics | |
| I missed face-to-face contact with my colleagues, so any long-term change to working practice needs to include some in-person contact | 1.22 (55) |
| I missed team working, so any long-term change to working practice should provide opportunity for team working | 0.98 (54) |
| The opportunity to work differently has been positive | 0.97 (63) |
| I have had to travel more than usual during the pandemic | 0.80 (56) |
| The COVID-19 situation gave me time/space to think about how my job could be done more effectively | 0.78 (64) |
| I have gained new skills and knowledge due to workplace changes during the COVID-19 pandemic | 0.74 (66) |
| I was unhappy that I had to take on different responsibilities/duties during this period | –0.70 (61) |
| I have been busier than normal during the COVID-19 pandemic | 0.67 (66) |
| I can be more productive on some tasks from home | 0.65 (55) |
| The chance to work in another area has made me consider changing my job | –0.61 (46) |
| The COVID-19 situation gave me time to tidy up my notes/office/clinical space or other admin and housekeeping things that have improved my working context | 0.44 (61) |
| I find online meetings (eg Skype/Microsoft Teams) more tiring than face-to-face meetings | 0.22 (49) |
| I have had a better work/home life balance during COVID-19 | 0.11 (66) |
| I was able to complete Agored [Wales education provider] training units or other learning activity due to the COVID-19 situation | 0.04 (56) |
Stressors and support during the COVID-19 pandemic
A majority (72% 49/68 weighted average 0.91) of staff experienced more work-related or overall (work and home) stress (76% 52/68, weighted average 0.97):
‘[I felt more] stressed towards the end of lockdown in relation to recommending services safely for staff and patients.’
‘[It is] still a very stressful and difficult time for work and family … Every day there has been something new to adapt to.’
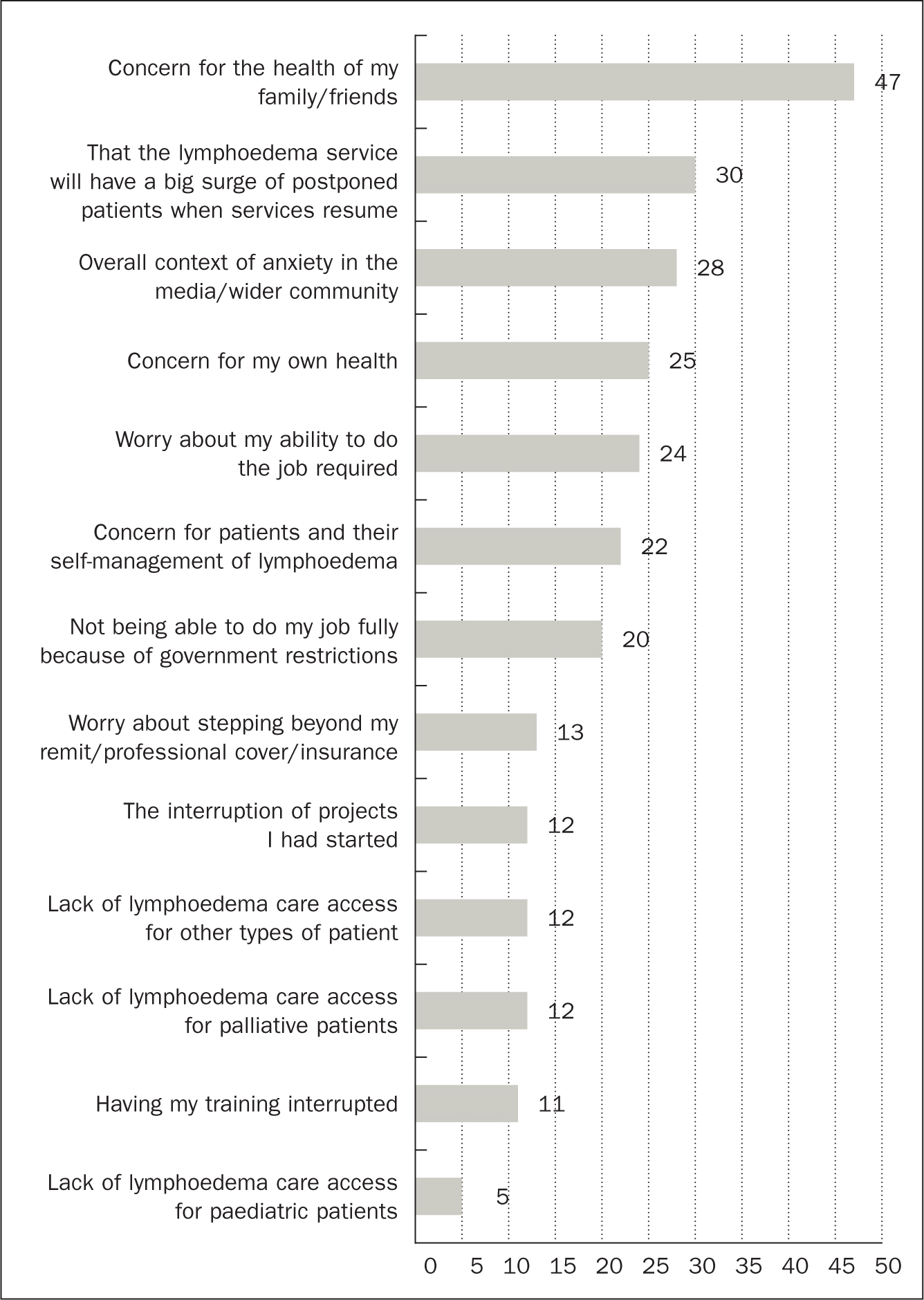
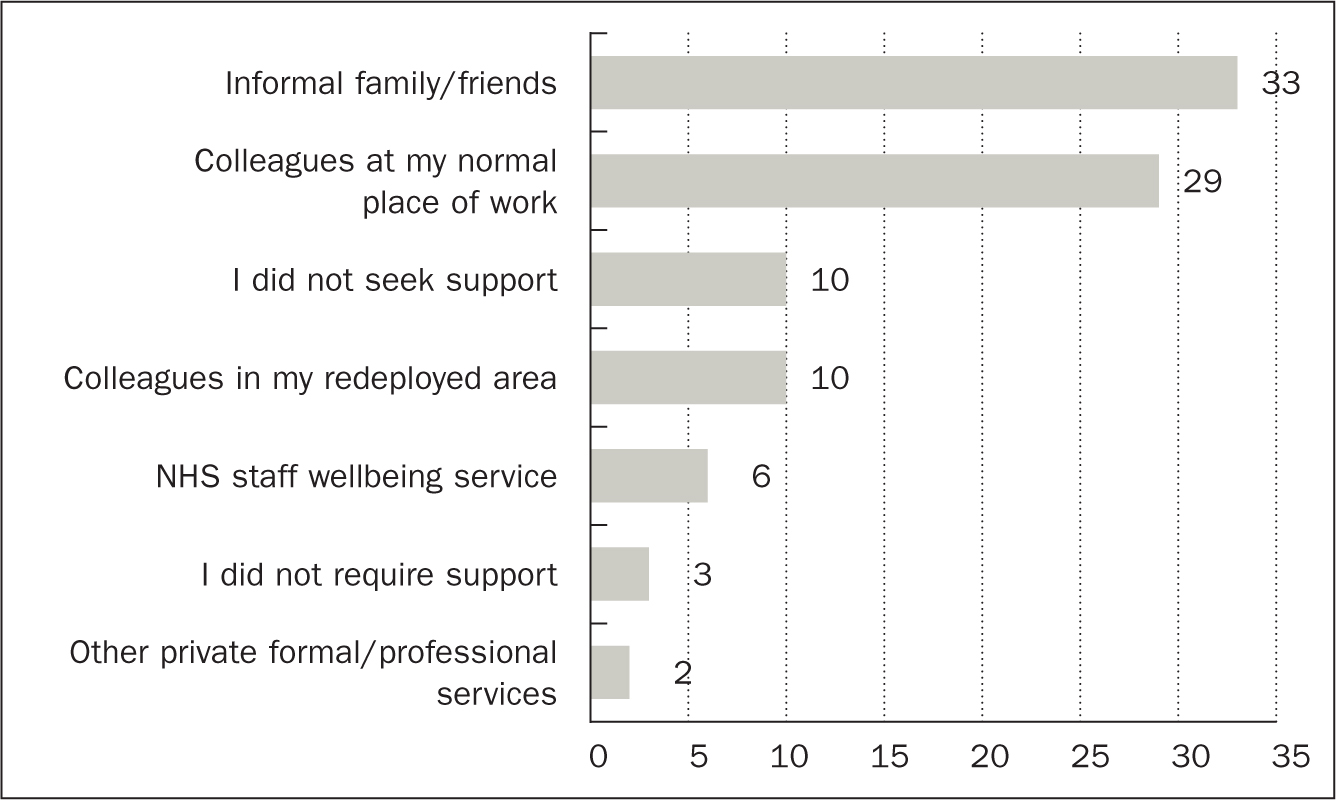
The health of family and friends was the main concern (Figure 2). With direct questioning, almost half the respondents felt guilty about not working ‘on the frontline’ with poorly patients (25/54). Informal sources of support were predominantly sought (Figure 3), but 10 respondents did not seek support. Having the Lymphoedema Network Wales national team placed in clinical areas of health boards helped foster a positive impact for more than half of respondents (57% 29/51; weighted average 0.80).
Lymphoedema services during the COVID-19 pandemic
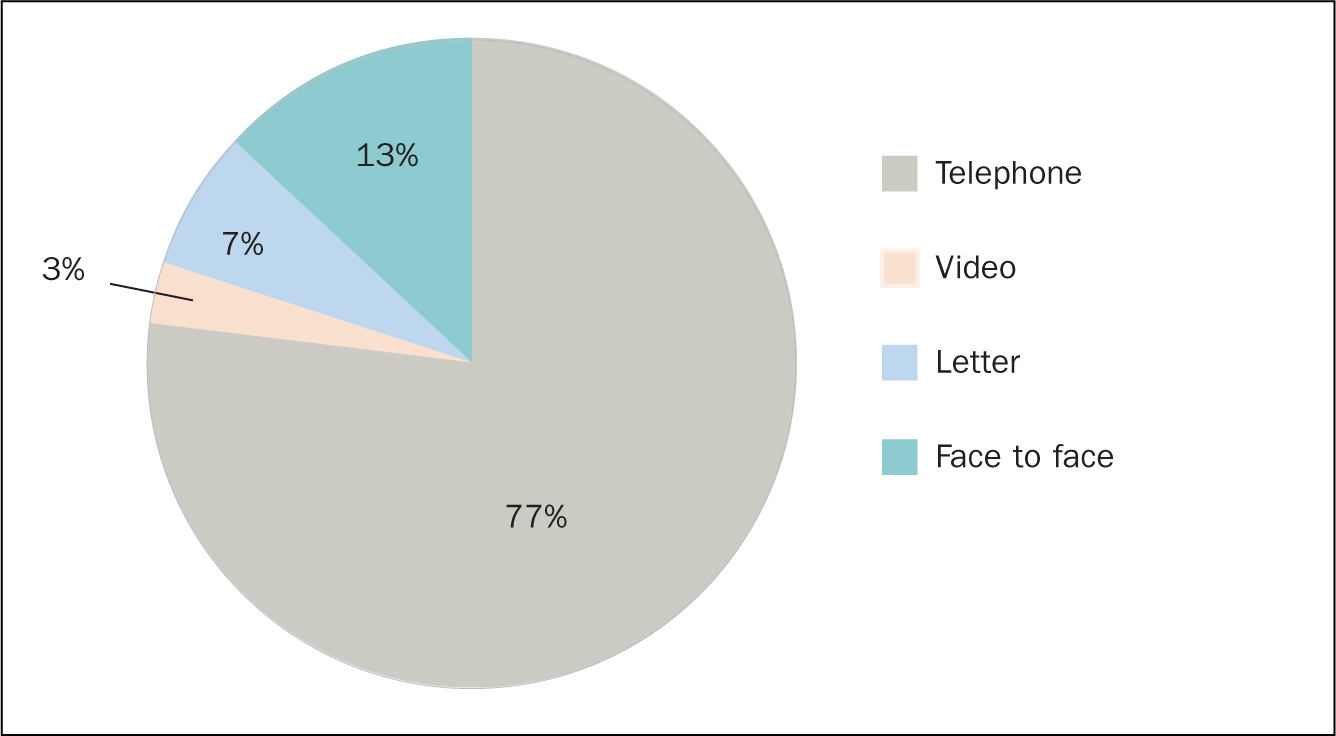
Lymphoedema services were sustained by 58 staff (40/68 not redeployed and 18/68 redeployed some of their time); 34 staff provided patient care, predominantly by telephone (77%). In addition, video calls were used for 3% of all patient contact (Figure 4). Half of staff (17/34) prescribed more patient education videos and 44% (15/34) shared more written material, including patient information leaflets, than usual. Comparing data from 2020 with the previous year, viewing of patient education video increased by 154% (1236 views versus 3142).
During the pandemic, home visit eligibility remained stable but intensive treatments were delayed and garments were posted from lymphoedema services rather than directly from companies (Table 2). Virtual care enabled value-based health care (VBH) optimising resource use in line with patient needs (Porter et al, 2013), narrowing the gap between need and demand (Gray, 2017), reducing unnecessary reviews and shortening follow-up consultation lengths. However, concerns were raised about patients being unable to access services if remote provision were increased (Table 2).
| Survey item | Weighted average strength of agreement (n) |
|---|---|
| Responses sorted by strength of agreement and disagreement. Strong differences are in bold and moderate differences in italics | |
| Providing garments and access to lymphoedema care | |
| It's a positive experience working with other healthcare professionals in managing patients with complex lymphoedema eg district nurses | 1.19 (47) |
| I have used the postal service more than usual for patients to access garments | 1.13 (30) |
| I have had to delay intensive treatment for lymphoedema patients | 1.06 (32) |
| I have used garment companies to deliver garments directly to the patient more often than usual | −0.72 (32) |
| I have used more garments from stock than I would normally | 0.32 (34) |
| I have done home visits to patients who would not have normally fallen within the criteria for a home visit | −0.19 (32) |
| Benefits of virtual services | |
| Virtual contact promotes value-based health care | 1.16 (32) |
| Virtual contact has shown me that I do not need to review patients as regularly as I did | 1.06 (33) |
| A virtual consultation for a follow-up patient is quicker than a face-to-face one* | 0.91 (33) |
| ‘Reducing the risk of lymphoedema’ assessment sessions could be virtual | 0.44 (32) |
| I have discharged more patients over the telephone than I would have normally | −0.33 (33) |
| All follow-ups could be virtual | −0.29 (34) |
| A virtual consultation for a new patient is quicker than a face-to-face one* | 0.15 (33) |
| We should continue with the first appointment being virtual/by phone after this current period | 0.12 (33) |
| Accessibility of virtual services | |
| Being hands-on when assessing all patients is essential | 0.58 (33) |
| I am extremely concerned about accessibility to the service for some patients if we increase our telephone/video ways of working | 0.06 (34) |
| I found doing the virtual/phone consultations difficult | −0.06 (34) |
Overall, virtual services (telephone/video contact) were considered most beneficial and suitable for risk reduction groups and patients with mild or moderate lymphoedema because they were able to self-manage the condition (Table 3). Patients with increasingly complex lymphoedema would also likely benefit but the suitability of virtual services for them was questioned (Table 3). Interestingly, the majority of staff assumed that fewer than 50% of patients on the existing caseload would happily continue with virtual services (<50%=25; >51%=9; range <10%–90%).
| Patient group | Benefit % (n) | Not suitable % (n) |
|---|---|---|
| Risk reduction | 62% (21/34) | 15% (5/34) |
| Mild | 85% (29/34) | 0% (0/34) |
| Moderate | 82% (28/34) | 3% (1/34) |
| Severe | 50% (17/34) | 24% (8/34) |
| Complex | 44% (15/34) | 44% (15/34) |
| Paediatrics* | 29% (10/34) | 26% (9/34) |
| Palliative | 32% (11/34) | 56% (19/34) |
| Domiciliary visits | 44% (15/34) | 35% (12/34) |
Virtual lymphoedema services during the COVID-19 pandemic
Three key benefits of virtual care were identified:
Many patients with lymphoedema were supported during COVID-19 shielding with virtual appointments. This enabled therapists to deliver VBH, prioritising need, justifying face-to-face contact and minimising waste:
‘Concerns can be dealt with on the day rather than needing to wait for an appointment. Triage need to attend clinic on the phone rather then just automatically bringing all patients into clinic.’
‘Ideal way to identify if clinic/home visits are required. If patients are happy or not to manage their lymphoedema at that time without clinic visits.’
‘If complex or palliative groups needed home visit as determined from tel call, this was done.’
‘Telephone contact with complex patients between face-to-face contacts might improve efficacy.’
Being able to reassure and offer advice, order compression garments and reiterate the cornerstones of care were seen as key benefits that may reduce complications:
‘[Patients] could still contact us and had support … [this] brought them back in line to the four cornerstones [and] discussions to prevent hospital admissions … Paediatrics supported parents in their management.’
‘[I could give] risk/early lymphoedema or mild/moderate … advice for self-management over the telephone more easily, [and patients] could measure own legs/arms etc.
‘Easier to manage, less likely to deteriorate, patients don′t have to worry about access/getting here.’
Challenges of virtual lymphoedema care
Three enablers and limiters of virtual care were described:
Lymphoedema can lead to complicated problems and deterioration, requiring dexterity and sensory skills to assess limbs and skin condition, which may render virtual care unsuitable for some:
‘[In cases of] skin changes and larger volumes, [you're] visually unable to assess tissue firmness, temp, and these measurements are [needed for care planning].’
‘Necessary to examine limbs, skin texture, skin damage and mobility levels.’
‘Paeds group can change quickly … Palliative patients can be offered support emotionally or through compression, which can ease their symptoms dramatically.’
‘People with more complex problems ie lymphorrhoea/wounds are difficult to [deal with] over the telephone.’
Compounding the assessment of complex or changing lymphoedema was the dearth of information garnered virtually. In particular, a reliance on symptom self-reporting was considered inadequate, burdensome and, potentially, misleading, and could leave patients at risk of deterioration:
‘Severe [cases] may need some input again. This is very individual—they may all require visual [assessment]. It is dependent on the patient's view of their condition’
‘[We] need to check these patients for changes at clinic … patients can see their lymphoedema differently to clinicians.’
‘What may well be nothing to them or not important to mention may be something that we pick up from having visually seen the patient.’
‘Not realistic to prescribe garments and antibiotics continually without measurements [based] on patients/family reporting.’
‘The teenager generation may be playing down their skin changes.’
Individualised care appears as both an overarching enabler and a limiter of virtual services. While virtual services were reviewed in terms of key patient groups, the need for an individualised approach based on patient circumstances and lymphoedema needs was paramount:
‘All patients benefit depending on their circumstances.’
‘Palliative and paediatric patients can benefit from a video/phone appointment where the needs of the patient and the input that is required from ourselves is appropriate to do so.’
‘Everyone is suitable but then a decision needs to be made [regarding the suitability of a virtual follow-up appointment] following the call.’
Staff views of the patient experience of virtual care
Staff felt patients may be more able to self-manage than previously presumed (65% 22/34). However, concerns of weight gain (66% 41/62; weighted average 0.66) were reported. Some patients did not expect to be contacted by phone by the lymphoedema services; however, all patients who were called during the COVID-19 pandemic responded positively, particularly those shielding:
‘Patients described anxiety/stress of a) not being able to attend [the outpatient department] b) being exposed to infection if they did … expressed relief re ongoing support and supply of garments.’
‘Most were delighted that the clinic had made the effort to contact them by phone. Those who needed urgent contact were relieved we could offer a limited service to them.’
A few negative patient experiences (12% 4/34) were reported and were typically based on single experiences regarding written communication and confusion, advice given or willingness to discuss matters over the telephone.
Discussion
This is the first evaluation to explore the impact of COVID-19 on lymphoedema staff and services using service-led scoping data. This evaluation garnered experiences of lymphoedema staff working in different services and from home. Supportive information technology was required to facilitate working and reduce stress at this difficult time. Being attentive to the needs of others was also important.
Unsurprisingly, anxiety was raised with the utmost concern for the health of friends and family (Nie et al, 2020) and unmet lymphoedema needs. However, team working and camaraderie fostered a united service and supportive working environment for many. Informal support was sought by many but some sought no support at all. The long-term effects on staff remain unknown. Psychological distress among health workers during this pandemic highlights the need for supportive psychological services (Zaka et al, 2020) and this evaluation supports that this applies equally to non-frontline workers (Li et al, 2020).
Virtual services were well received by patients (Elwell and Sneddon, 2020), and replaced many of the traditional face-to-face appointments during the pandemic. Virtual care presents a challenging opportunity for health services to thrive in the face of adversity and as an approach to VBH. However, it was difficult to assess complex patient information without visual information, and the reliance on patient description alone was a challenge and patients could provide potentially spurious data, albeit with good intentions. The main limitation—the lack of sensory data—was in keeping with other reports for telephone-based services (Elwell and Sneddon, 2020).
Owing to the sparse use of video appointments (3% of contact), respondent information could not be used to explore reasons for limited update. However, lymphoedema services have since increased video-based appointments through procurement of a secure web-based platform, with anecdotal reports showing ease of use and timely access.
The benefits and suitability of virtual lymphoedema care were considered from the perspective of the therapist as a patient advocate, offering key considerations to maintain equitable, safe and high-quality lymphoedema assessment, triage and care. Many of the considerations warrant future evaluations, particularly around maintaining equity and the quality of remote assessments (Galiano-Castillo et al, 2014; Elwell and Sneddon, 2020), in addition to flexible use of virtual services based on patient preference and healthcare need, along with service demand and capacity (Smith et al, 2020). Staff reported that virtual services enabled triage and prioritisation of patient contact, but discharge rates observed remained unchanged. Long-term follow-up will help identify some of the delayed impacts, limiters and enablers: is virtual care more than a ‘make do’?
This study highlights the importance of lymphoedema care in all NHS sectors, along with the value of team working and supportive environments instilling the values of the Nursing and Midwifery Council (2018): prioritise people, practice effectively, preserve safety, promote professionalism and trust. Overwhelmingly, staff strove to improve quality and safety of evidence-based lymphoedema care and knowledge beyond the current pandemic.
To empower patients, healthcare workers themselves must feel empowered (Hewitt, 2002). This evaluation enabled staff to anonymously contribute to service development. Respondents identified opportunities for learning and education for both staff being redeployed and workers in the services where they were moved. Lymphoedema experts in primary and secondary care supported the cornerstones of lymphoedema care in their new area.
Respondents recognised the need for components of patient advocacy—communication, competency, sensitivity and patient empowerment (Vaartio et al, 2006)—in everyday lymphoedema care. Given the unprecedented times and the heightened burden of COVID-19 for vulnerable groups, advocacy as a patient right and duty of providers is paramount.
Limitations
Owing to the volume of patient research under way, this study focused on the experience of lymphoedema staff and services, with some second-hand reports of patient experience.
The majority of virtual lymphoedema care was provided by telephone but respondents were asked to consider virtual services combining video and telephone. Messaging services were not explored. Data are reported on an all-Wales basis, negating any assessment of the impact of rurality.
Conclusion
Overall, lymphoedema staff adapted to new roles with supportive colleagues and training. However, a majority also reported increased stress.
Lymphoedema services across Wales were well prepared to deliver virtual services owing to ongoing efforts to develop VBH through documentation and prioritisation tools, including patient-reported outcome measures. Notably, the majority of virtual care was provided by telephone; however, video-based appointments have increased since the evaluation.
This paper identifies opportunities for lymphoedema services and staff to thrive, using virtual services to streamline efficient working and ensure patients are ‘seen’ at a time and place when needed. However, the need for team working, in-person contact and tactile patient assessment remained for many. More research is needed to understand the long-term impact of virtual lymphoedema care, including video-based appointments.