
The Dutch philosopher, Desiderius Erasmus, is attributed as first coining the phrase ‘prevention is better than cure’. Nowhere has this maxim been more applicable than in the field of dementia care, where curative treatment options remain frustratingly elusive. This is particularly worrying given the stark epidemiological evidence for the condition. Globally, about 50 million people have dementia, with nearly 10 million new cases every year (World Health Organization, 2019). In relation to the UK, there are an estimated 850 000 people with dementia, with numbers set to rise to over 1 million by 2025 (Alzheimer's Society, 2019a). Notably, deaths due to dementia and Alzheimer's disease increased for the third consecutive year in 2017 and it remained the leading cause of mortality in England and Wales, accounting for 12.7% of all deaths registered (Office for National Statistics, 2018). The Lancet Commission on Dementia urges health professionals to be ambitious about prevention, arguing that pushing back the age of dementia onset would bring enormous benefits, since it has been suggested that a delay in onset of 1 year could prevent more than 9 million cases of dementia by 2050, and a delay in onset of 5 years could halve the prevalence of dementia globally (Livingston et al, 2017).
While there is greater understanding of the pathophysiology of Alzheimer's disease, its causation has yet to be fully uncovered and it is likely to be multifactorial; age and genetics are certainly implicated. Medical conditions, such as stroke, diabetes and hypertension, may also contribute to an increased risk of Alzheimer's disease and its subsequent disease course (Edwards et al, 2019). More recently, there has been increasing evidence of other potentially modifiable risk factors (MRFs), including nutrition (Antal et al, 2017), physical exercise (Brini et al, 2018), social engagement (Hersi et al, 2017), cognitive stimulation (Yates et al, 2016), smoking (Durazzo et al, 2014) and alcohol consumption (Ballard and Lang, 2018), which appear to play a significant role. Alongside this, the evidence base relating to the prevention of dementia has been accumulating steadily. In 2014, the World Dementia Council asked the Alzheimer's Association to evaluate and report on the state of the evidence on MRFs for cognitive decline and dementia, and a summary of this evaluation was subsequently published by Baumgart et al (2015), in which the authors assert that the issue of addressing MRFs for dementia can no longer solely be a matter of academic discussion, but requires action. Consistent with this, the Department of Health and Social Care (DHSC) (2018) has recently outlined its vision for prevention, which affirms that we can make healthy lifestyle choices to reduce our chances of getting conditions such as dementia.
In keeping with these calls for action, a multidisciplinary advisory group of health professionals involved in dementia care was convened in January 2018 in the UK to review the current evidence base regarding MRFs for early Alzheimer's disease and mild cognitive impairment (MCI), and to generate a user-friendly aide memoire to assist positive interventions in the clinical arena. The advisory group comprised seven individuals from a variety of disciplines, including a consultant geriatrician, dietitian, clinical specialist physiotherapist, consultant nurse for dementia, clinical nurse specialist in older persons' mental health, lecturer in psychology, and specialist in dementia education. During the meeting, the advisors discussed evidence from published literature and their clinical experience of working in dementia, and reached agreement on the issues and recommendations they considered were most important. This article is an outcome of that meeting, its objectives being to raise awareness of the issues that are most applicable to nurses, and to provide practical guidance on how nurses may actively seek to address MRFs for early Alzheimer's disease and MCI in clinical practice.
Modifiable risk factors for early Alzheimer's disease and mild cognitive impairment
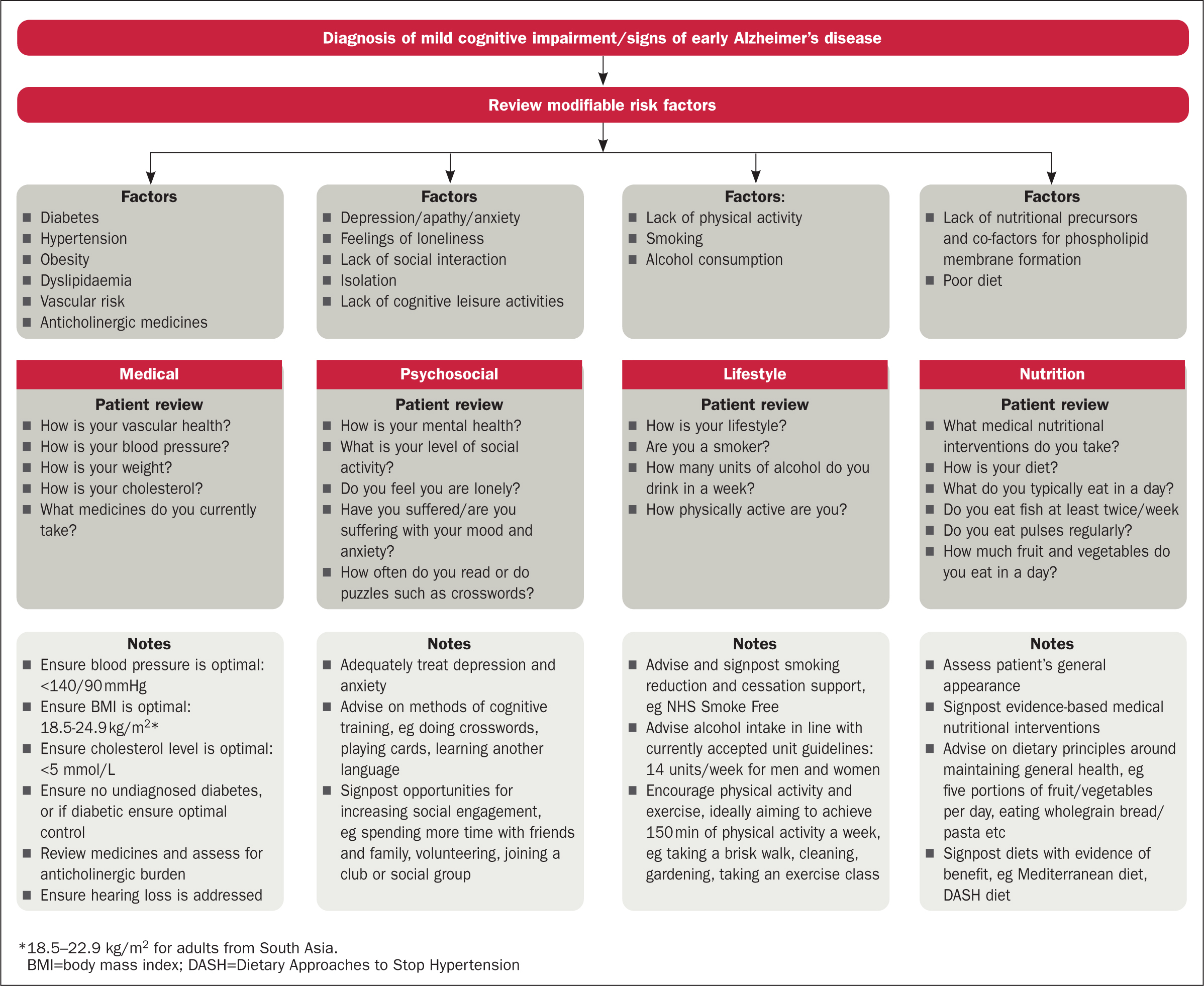
Based on their assessment of the published literature and personal experience, the advisors determined that MRFs for early Alzheimer's disease and MCI fall broadly into four areas where there is evidence to support interventions that may help delay cognitive decline or reduce the risk of developing the disease. These areas are categorised as medical, psychosocial, lifestyle and nutrition (Table 1). What follows is a summary of the key evidence identified and discussed by the panel relating to each of these categories.
Table 1. Modifiable risk factors for early Alzheimer's disease and mild cognitive impairment, by domain
| Domain | Risk factors |
|---|---|
| Medical |
|
| Psychosocial |
|
| Lifestyle |
|
| Nutrition |
|
Medical
There is evidence for a link between a number of cardiovascular risk factors and dementia. Such risk factors include diabetes, mid-life hypertension, obesity and mid-life hyperlipidaemia. Other factors categorised within the medical domain include anticholinergic medications and hearing loss.
Evidence has shown a greater likelihood of individuals with diabetes having lower cognitive performance and an increased risk of dementia, concluding that the association between diabetes and dementia appears strong, although it is inconclusive (Baumgart et al, 2015). Furthermore, Baumgart et al (2015) cite a meta-analysis that demonstrated that individuals with MCI and diabetes were more likely to progress to dementia than those with MCI and no diabetes (Cooper et al, 2015). Some evidence suggests that diabetes increases dementia risk not only through vascular pathways but also through the interactions of other biological mechanisms related to diabetes itself, such as insulin resistance, impaired glucose metabolism, the presence of advanced glycation end products and β-amyloid formation (Mushtaq et al, 2014).
A systematic review of meta-analyses, observational studies and randomised controlled trials found that treatments for hypertension (in particular, calcium channel blockers and renin-angiotensin system blockers) may reduce the risk of cognitive decline and dementia (Rouch et al, 2015).
Evidence from several meta-analyses, systematic reviews and individual prospective studies has demonstrated that mid-life obesity is associated with an increased risk of dementia (Baumgart et al, 2015). Furthermore, Dye et al (2017) reported that, in addition to an increased risk of an accelerated cognitive decline with ageing, there is evidence to suggest that obesity in early-to-mid adulthood may have an immediate detrimental impact on cognitive functioning (Dye et al, 2017).
Research into a potential link between hyperlipidaemia (elevated cholesterol) in mid and late life and the risk of dementia has yielded inconsistent findings, and no association between hyperlipidaemia and vascular dementia has been found (Baumgart et al, 2015). A meta-analysis of evidence for an association between serum cholesterol and the risk of late-life dementia, derived from over 23 000 subjects from 17 studies, led to the conclusion that high mid-life total cholesterol increases the risk of late-life Alzheimer's disease, but the study also acknowledged that significant gaps in the evidence remain (Anstey et al, 2017). Observational studies of patients taking statins have seemed to show a reduction in the risk of dementia, although more robust cohort studies have thus far failed to reproduce these findings (Baumgart et al, 2015). Moreover, a Cochrane review of randomised, double-blind, placebo-controlled trials, in which people at risk of dementia were treated with statins for at least 12 months, concluded that statins given in later life to people at risk of vascular disease do not prevent cognitive decline or dementia (McGuinness et al, 2016).
It is widely acknowledged that anticholinergic medications have a detrimental impact on cognitive performance (Richardson et al, 2018; López-Álvarez et al, 2019). Due to increasing health complications in later life, the use of polypharmacy in elderly people is high, and many commonly prescribed drugs have anticholinergic effects, including neuropsychiatric drugs (eg tricyclic antidepressants, antipsychotic agents, anti-epileptic drugs, antiparkinsonian medication) and a range of non-psychoactive drugs (eg antihistamines, antispasmodics, anti-ulcer agents, bronchodilators, diuretics, corticoids, cardiovascular medications) (López-Álvarez et al, 2019). A UK case-control study conducted in over 40 000 patients with dementia aged 65–99 years and approximately 284 000 control subjects without dementia found that dementia was associated with an increasing average anticholinergic cognitive burden (ACB) score, and a strong association between some classes of anticholinergic drugs (eg antidepressants, urological agents, and antiparkinsonian drugs) and future dementia incidence (Richardson et al, 2018). Similarly, a large nested case-control study, conducted in more than 280 000 patients with a diagnosis of dementia and matched controls, clearly demonstrated that exposure to several types of strong anticholinergic drugs (including antidepressants, antiparkinsonian agents, antipsychotic medications, and anti-epileptic drugs) is associated with an increased risk of dementia, the association being particularly strong in those diagnosed before the age of 80 years (Coupland et al, 2019).
Age-related hearing loss is associated with the risk of developing dementia (Uchida et al, 2019). In a cross-sectional analysis of the English Longitudinal Study of Ageing (ELSA), participants who had self-reported or objectively assessed moderate and poor hearing were more likely to have a dementia diagnosis than those with normal hearing, after adjusting for potential confounders (Davies et al, 2017). Longitudinally, when compared with those with normal hearing, the hazard of developing dementia was about 40% higher in individuals who self-reported moderate hearing (hazard ratio, 1.39; 95% confidence interval, 1.01–1.92) and about 60% higher in those who self-reported poor hearing (hazard ratio, 1.57; 95% confidence interval, 1.12–2.02) (Davies, 2017). In a further cross-sectional analysis of ELSA, the association between objectively measured hearing loss and poor cognition was seen only in individuals with untreated hearing loss (ie those who did not use hearing aids), and social isolation appeared to mediate the association, leading the authors to conclude that cognitive decline associated with age-related hearing impairment is likely to be preventable by increased screening in the elderly and early rehabilitation (Ray et al, 2018). In a meta-analysis of 36 studies involving more than 20 000 participants, a small but significant association was found for age-related hearing loss within all domains of cognitive function, and significant associations were found between age-related hearing loss and both cognitive impairment and dementia (Loughrey et al, 2018). Age-related hearing loss therefore represents an MRF and possible biomarker for cognitive decline, cognitive impairment, and dementia (Loughrey et al, 2018).
Psychosocial
Several psychosocial factors have been identified as being associated with dementia, and these may therefore represent potential MRFs for early Alzheimer's disease and MCI. These not only include psychiatric conditions, such as depression, but also social factors, including social engagement, cognitive stimulation and loneliness.
The risk of dementia has been found to be higher among individuals with depression and there appears to be a link between cognitive decline and symptoms of depression (Mirza et al, 2016). However, it is not entirely clear whether depression is a risk factor for dementia, or an early indication of changes associated with the condition. Barnes et al (2012) conducted a large retrospective cohort study of more than 13 500 members of a medical care programme who underwent a voluntary multiphasic health check-up, and found that there was an increased risk for dementia among those with mid-life and late-life depression (Barnes et al, 2012). When they examined the incidence of Alzheimer's disease and vascular dementia separately, subjects who only had late-life depressive symptoms had a twofold increase in the risk of Alzheimer's disease, whereas those with both mid-life and late-life symptoms had more than a threefold increase in the risk of vascular dementia (Barnes et al, 2012).
Public Health England (PHE) (2016) reported that data from 22 studies that included more than 29 000 participants demonstrate a 46% lower risk of dementia among people with high levels of mental activity in comparison with those with low mental activity. The authors of the report argue that being socially active can help reduce the risk of dementia by improving mood, relieving stress, reducing the risk of depression and reducing loneliness (PHE, 2016). The Alzheimer's Society (2019b) refers to the maxim ‘use it or lose it’ when recommending that a daily ‘brain workout’, using puzzles, word searches or crosswords, might help reduce the risk of dementia. Similarly, learning a new language may equip the brain with resources that make it more resilient to brain diseases such as the dementias (Alzheimer's Society, 2019b). A Cochrane review identified many randomised controlled trials of mental engagement/cognitive training interventions that have demonstrated improvements in immediate and delayed recall among those in the treatment group compared with controls (Martin et al, 2011).
In an analysis of data from the Health and Retirement Study, which included over 12 000 participants who were followed up for 10 years, loneliness was found to be associated with a 40% increased risk of dementia (Sutin et al, 2018). This association was found to be independent of social isolation (living alone, unmarried, without social support), reflecting similar findings from other studies, which have reported that feelings of loneliness, rather than social isolation, predict dementia onset (Holwerda et al, 2014).
Lifestyle
In addition to psychosocial factors, several lifestyle factors have been identified as important MRFs for dementia.
Physical activity has a range of health benefits, including contributing to a reduced risk of cerebrovascular and cardiovascular diseases, such as diabetes, obesity and hypertension. In a review of the evidence for the benefits of regular exercise, Ahlskog et al (2011) concluded that ongoing, moderate-intensity physical exercise should be recommended for all ages as a means of lowering cognitive risk and slowing cognitive decline. A more recent systematic review and meta-analysis of longitudinal studies on the relationship between physical activity and the risk of cognitive decline, all-cause dementia, Alzheimer's disease and vascular dementia confirmed the importance of physical activity as an MRF—it found that high physical activity is more protective against Alzheimer's disease (odds ratio [95% confidence interval], 0.62 [0.49, 0.75]) than it is against cognitive decline (0.67 [0.55, 0.78]) and all-cause dementia (0.79 [0.69, 0.88]), and non-protective against vascular dementia (0.92 [0.62, 1.30]) (Guure et al, 2017).
Cardiovascular disease, stroke, diabetes, hypertension and hypercholesterolaemia have been individually cited as MRFs for Alzheimer's disease and vascular dementia (Gottesman et al, 2017; Ngandu et al, 2015) and, because smoking is linked with increased risk for the development of these conditions, it follows that smoking is also an MRF, regardless of any evidence of a direct link to dementia. Consistent with this, a systematic review of published studies (Durazzo et al, 2014) concluded that the cumulative body of research indicates that previous and active smoking is associated with a significantly increased risk for Alzheimer's disease.
The effect of alcohol consumption on the risk of dementia is less clear. Studies suggest a U-shaped relationship between regular alcohol consumption and cognitive function: frequent heavy consumption decreases cognitive performance, whereas regular light and moderate consumption may have a protective impact (Gutwinski et al, 2018). Chronic heavy alcohol consumption can cause thiamine (vitamin B1) deficiency and lead to Korsakoff's syndrome, characterised by symptoms including confabulation, disorientation, severe memory loss and amnesia (Arts et al, 2017; Rehm et al, 2019; Wiegmann et al, 2020).
Nutrition
Maintaining a healthy diet is beneficial for any patient. The NHS (2018) advocates eating at least five portions of a variety of fruit and vegetables every day, based on advice from the World Health Organization (2005), which recommends eating a minimum of 400 g of fruit and vegetables a day to lower the risk of chronic conditions, such as heart disease, cancer, diabetes, and obesity. Emerging evidence suggests that maintaining a healthy diet can protect against cognitive decline, possibly due to associated reductions in cardiovascular risk factors (Scarmeas et al, 2006; Morris et al, 2015; Vandewoude et al, 2016; Berendsen et al, 2017; Cherbuin and Walsh, 2019). Such diets include the Mediterranean diet, which can be broadly described as one containing relatively little red meat, with a focus on including whole grains, fruits and vegetables, fish, nuts and olive oil. A systematic review (Petersson and Philippou, 2016) indicated that subjects who had a high Mediterranean diet score (ie those who consumed a diet almost entirely of this nature) had a reduced risk of cognitive decline.
Because hypertension is a potential MRF for dementia, diets that specifically target hypertension may also have relevance in reducing the risk of dementia. The Dietary Approaches to Stop Hypertension (DASH) eating plan (Sacks et al, 1999) requires no special foods, but provides daily and weekly nutritional goals, and recommends eating vegetables, fruits, whole grains, fat-free or low-fat dairy products, fish, poultry, beans, nuts and vegetable oils (Association of UK Dietitians, 2017; Mayo Clinic 2019). Foods that are high in saturated fat, and sugar-sweetened beverages and sweets, are limited. A systematic review and meta-analysis demonstrated that the DASH diet can have a beneficial impact on blood pressure in adults, significantly reducing systolic blood pressure by 6.74 mmHg (95% confidence interval, -8.25, -5.23) and diastolic blood pressure by 3.54 mmHg (95% confidence interval, -4.29, -2.79) (Saneei et al, 2014). Since diabetes, pre-diabetes and high ‘normal’ blood glucose levels have also been linked to neurodegenerative processes, diets that limit carbohydrate intake have also been proposed as a potential preventive tool (Wlodarek et al, 2019).
Effective dietary interventions can have far-reaching implications for public health, especially with the growing burden of dementia in an ageing population. High-quality diets, such as the Mediterranean and DASH diets, can be further modified and simplified, such as in the Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet, to provide better protection against dementia (Morris et al, 2015). The MIND diet, for instance, emphasises the dietary components and servings linked to neuroprotection and dementia prevention, but promotes lower servings than those specified for the DASH or Mediterranean diet (Morris et al, 2015), which can potentially improve adherence.
Synaptic loss is an important feature of early Alzheimer's disease and the formation of new synapses is dependent on key nutritional elements that are known to be deficient in people with the disease, such as omega-3 fatty acids (Jicha and Markesbery, 2010), folate and vitamins B12, C and E (Glasø et al, 2004; Smach et al, 2011), as well as other important micronutrients (Scheltens et al, 2012). There has therefore been a growing interest in recent years in nutritional supplementation as a way to maintain a ‘healthy brain’ and reduce cognitive decline (Vandewoude et al, 2016). Previous studies have looked at a range of nutritional factors to modify clinical progression of Alzheimer's disease (Le Bars et al, 1997; Freund-Levi et al, 2006; Smith et al, 2010; Jernerén et al, 2015; Charemboon and Jaisin, 2015).
While the correction of specific deficiencies is necessary to improve nutritional status, currently there is no generally applicable evidence to recommend the use of single-agent micronutrient supplementation at any stage of dementia or for prevention (Vandewoude et al, 2016; Rutjes et al, 2018). Conversely, there is emerging evidence that supplementation with a combination of such micronutrients may be more promising, consistent with the fact that a deficiency in any precursor has the potential to be a rate limiting step in the Kennedy cycle, the biochemical pathway involved in the synthesis of phospholipids required for the formation of neuronal membranes and synapses (Sakamoto et al, 2007; Rasmussen, 2019).
An example of such a multi-nutrient combination, which has been tested in the clinical trial setting, is Fortasyn Connect—a combination of docosahexaenoic acid; eicosapentaenoic acid; uridine monophosphate; choline; vitamins B12, B6, C, E, and folic acid; phospholipids; and selenium (van Wijk et al, 2014). Souvenaid, which contains the nutritional combination Fortasyn Connect, is described by the manufacturer as ‘a food for special medical purposes for the dietary management of early Alzheimer's disease’. Two previous randomised clinical trials in patients with mild Alzheimer's disease dementia reported that daily intake of Fortasyn Connect for 3 or 6 months improved memory performance (Scheltens et al, 2010; 2012). LipiDiDiet, which was the first randomised, controlled, double-blind trial in prodromal Alzheimer's disease, showed that Fortasyn Connect had no significant effect on the primary endpoint of cognitive performance using a neuropsychological test battery over 2 years (Soininen et al, 2017). However, it demonstrated significant benefit on secondary endpoints, including domains of cognition affected by Alzheimer's disease and hippocampal atrophy. It is anticipated that an intervention such as this would take time to have an effect and would benefit people earlier in their disease course. Multi-nutrient supplementation during early Alzheimer's disease, either alone or in combination with other prevention strategies, may therefore warrant further investigation.
Interventions aimed at targeting modifiable risk factors
There is clearly a strong and developing evidence base relating to the role of MRFs in the aetiology of early Alzheimer's disease and MCI. What is also clear is that this is a multifactorial issue, there being no single key factor to target for reducing the risk of cognitive decline, dementia and the disease. Consequently, the advisory group sought to make recommendations that support a multi-domain approach to intervention. In so doing, it agreed on a range of pragmatic interventional approaches that fall within the remit of health professionals in general, and nurses in particular. These interventions are presented below as they relate to the four domains identified earlier (see also Figure 1). Additional resources relating to these domains are provided in Box 1.
Box 1.Additional resources
| Medical | www.alzheimers.org.uk/about-dementia/risk-factors-and-prevention/how-reduce-your-risk-dementia www.nhs.uk/conditions/high-blood-pressure-hypertension www.nice.org.uk/guidance/ng136 www.nhs.uk/conditions/high-cholesterol/ www.bhf.org.uk/informationsupport/heart-matters-magazine/research/blood-pressure/blood-pressure-tips www.nice.org.uk/guidance/cg181 www.nhs.uk/live-well/healthy-weight/height-weight-chart www.nhs.uk/news/obesity/weight-link-to-dementia www.alzheimers.org.uk/news/2018-04-10/study-suggests-links-between-hearing-loss-and-dementia-alzheimers-society-comment www.ACBcalc.com |
| Psychosocial | www.alzheimersresearchuk.org/social-engagement-associated-better-cognition-age-50 www.dementiamatters.net/living-with-a-dementia-diagnosis www.nhs.uk/conditions/dementia/activities www.alzheimers.org.uk/research/our-research/have-go-brain-training www.alzheimers.org.uk/about-dementia/symptoms-and-diagnosis/apathy-depression-anxiety |
| Lifestyle | www.nhs.uk/live-well/exercise/free-fitness-ideas www.alzheimers.org.uk/about-dementia/risk-factors-and-prevention/how-reduce-your-risk-dementia www.nhs.uk/live-well/exercise/exercise-health-benefits www.nhs.uk/smokefree www.alzheimers.org.uk/about-dementia/risk-factors-and-prevention/smoking-and-dementia www.nhs.uk/news/neurology/smoking-linked-to-alzheimers-risk www.bhf.org.uk/informationsupport/support/healthy-living/healthy-eating/alcohol www.alzheimers.org.uk/about-dementia/risk-factors-and-prevention/alcohol www.gov.uk/government/publications/communicating-the-uk-chief-medical-officers-alcohol-guidelines |
| Nutrition | www.nhs.uk/live-well/eat-well/the-eatwell-guide www.gov.uk/government/publications/the-eatwell-guide www.alzheimers.org.uk/about-dementia/risk-factors-and-prevention/how-reduce-your-risk-dementia www.nhs.uk/live-well/eat-well/what-is-a-mediterranean-diet www.mayoclinic.org/diseases-conditions/alzheimers-disease/expert-answers/alzheimers-disease/faq-20058062 https://dashdiet.org/what-is-the-dash-diet.html www.mysouvenaid.co.uk www.nutricia.co.uk/medical-nutrition/memory-loss-and-early-alzheimers-disease www.carersuk.org/help-and-advice/health/nutrition/dementia-and-nutrition |
Interventions related to medical factors
- Ensure blood pressure is optimal:
- Has the person had their blood pressure checked recently?
- Is there awareness that optimal blood pressure is less than 140/90 mmHg?
- Does the person need signposting to their GP for current blood pressure reading?
- Ensure body mass index (BMI) is optimal:
- A BMI of 18.5–24.9 kg/m2 (18.5–22.9 kg/m2 for adults from South Asia) is considered to be in the healthy weight range. A BMI of less than 18.5 kg/m2 is considered low and the person may require dietary advice
- Ensure cholesterol level is optimal:
- Has the person had their cholesterol checked recently? This should be ≤5 mmol/L for healthy adults
- Ensure there is no undiagnosed diabetes or, if the person has diabetes, ensure control is optimal for age
- Review medicines and assess for anticholinergic cognitive burden (ACB):
- When did the person last have a review of their current medication?
- Does the person know they can make an appointment with their GP or pharmacist to discuss their medication?
- Calculating the potential ACB in patients can be easily facilitated by using a recognised scale, such as the ACB Calculator (www.ACBcalc.com)
- Ensure any hearing loss is addressed. Regular hearing checks are recommended
Interventions related to psychosocial factors
- Adequately treat depression and anxiety:
- Many of the things that can cause people to feel depressed can also cause them to feel anxious, and vice versa
- Identification and treatment of depression is best enabled by the person's GP and/or mental health professionals. However, the starting point is often a recognition by the person: the simple act of asking someone how their mood is can be an important trigger
- Signpost opportunities for increasing social engagement:
- Being socially active can help reduce the risk of dementia by improving mood, relieving stress, reducing the risk of depression and reducing loneliness
- Encourage the person to try to keep in touch with the people who are important to them, such as friends and family. Volunteering, or joining a club or community group, are also good ways to stay socially active
- Health professionals can have a significant role for signposting opportunities to increase social engagement, but this is reliant on some form of assessment of the person's level of social activity
- Advise on methods of cognitive training:
- There is increasing evidence that daily ‘brain workouts’ such as doing puzzles, word searches or crosswords, playing cards or learning something new, such as another language, can help reduce the risk of dementia (Yates et al, 2016; Fissler et al, 2018)
Interventions related to lifestyle factors
- Encourage physical activity and exercise:
- Physical activity has a range of health benefits, including contributing to a reduced risk of heart attacks and stroke, diabetes, obesity and dementia. It also has a positive impact on mood and mental wellbeing
- Encourage the person to try to take regular physical activity: this may be a brisk walk, cleaning or gardening. It may be as little as 10 minutes a day, building up over time. Ideally, individuals should aim to achieve 150 minutes of physical activity a week, which can be spread out over the day and throughout the week into bite-size pieces
- Local leisure centres may well be offering initiatives such as free exercise classes or a free swim on certain days of the week to encourage people to get in shape. The NHS website Get Fit for Free is a useful starting point (www.nhs.uk/live-well/exercise/free-fitness-ideas)
- Advise and signpost smoking reduction and cessation support:
- Smoking has been linked to an increased risk of heart and lung conditions, diabetes and cancers. These are all known risk factors for developing Alzheimer's disease and vascular dementia
- Health professionals can play a pivotal role in assisting individuals to consider giving up smoking. Importantly, they can signpost comprehensive support resources such as NHS Smoke free (www.nhs.uk/smokefree/)
- Advise alcohol intake in line with current accepted unit guidelines:
- Current guidelines state that men and women should not drink more than 14 units of alcohol each week
- One unit of alcohol is measured as 10 mL or 8 g of pure alcohol, equating, approximately, to one 25 mL single measure of whisky (alcohol by volume (ABV) 40%), a third of a pint of beer (ABV 5–6%) or half a standard (175 mL) glass of red wine (ABV 12%).
Interventions related to nutritional factors
- Advise on dietary principles around maintaining general health:
- Current thinking points to aiming for five portions of fruit and vegetables a day (https://www.nhs.uk/live-well/eat-well/why-5-a-day) (NHS website, 2018). Protein, such as oily fish, beans, pulses, eggs or lean meat, should be consumed at least twice a day
- Limit sugar intake and be aware of hidden salt. Starchy foods, such as bread, potatoes and pasta, are recommended, as are wholegrain varieties, wherever possible
- Saturated fat intake should be limited
- 1.2 L (approximately six to eight glasses) of fluid (such as water, lower-fat milk and sugar-free drinks) a day is considered optimal
- This advice aligns closely with the Mediterranean-style diet, which is characterised by eating plenty of fruit, vegetables, legumes and cereals; it includes oily fish in the diet; eating less meat; choosing products that are low in sugar and saturated fat; choosing products made from vegetable and plant oils, such as olive oil; and having moderate alcohol intake
- Signpost evidence-based nutritional supplements:
- As with medication, many people can find themselves taking a cocktail of nutritional supplements. A review with some rationalisation of such intake might be of benefit, given the ambiguity of the evidence base
- In people who have received a diagnosis of Alzheimer's disease or MCI, Souvenaid may be helpful. Souvenaid is ‘a food for special medical purposes for the dietary management of early Alzheimer's disease’ and must be used under the supervision of a health professional. It contains Fortasyn Connect and needs to be purchased by the individual.
Conclusion
Nurses occupy a position of trust in society and are ideally placed to offer information and advice to those for whom they care. The potential for population-based health gains is nowhere more potent than in regard to the prevention of dementia. Nurses are ideally placed to offer advice in this area and this article has aimed to provide the rationale for such action. Additionally, it seeks to raise awareness among nurses so that barriers to addressing this increasingly important area of health promotion are lowered. We hope that nurses, assisted by reference to the evidence-based interventions spanning four major domains, will gain confidence to increasingly use their discussion/conversations with patients around lifestyle choices and changes so that MRFs for early Alzheimer's disease and MCI are addressed directly. In so doing, nurses will play an important role in helping to address this growing healthcare challenge.
KEY POINTS
- A multidisciplinary advisory group of health professionals involved in dementia care came together to discuss and assess the current evidence base regarding modifiable risk factors (MRFs) for early Alzheimer's disease and mild cognitive impairment
- MRFs in four areas were identified where there is evidence to support interventions that may help delay cognitive decline or reduce the risk of developing the disease—medical, psychosocial, lifestyle, nutrition
- Practical approaches through which health professionals, including nurses, can help to address MRFs in these four areas were developed
- Nurses are ideally placed to proactively help patients mitigate the risks of cognitive decline and the development of Alzheimer's disease
CPD reflective questions
- How do you think the phrase ‘prevention is better than cure’ relates to dementia care today?
- In terms of the current evidence base, what types of modifiable risk factors (MRFs) are associated with early Alzheimer's disease and mild cognitive impairment (MCI)?
- Which of these MRFs do you think are most relevant to the patients whom you see in your everyday practice?
- As a nurse, what steps can you take/what advice can you give to help address MRFs for early Alzheimer's disease and MCI in your patients?