

An electrocardiogram (ECG) is a recording of the electrical activity within the heart muscle and is the most commonly performed cardiac test (Kligfield et al, 2007). ECG monitoring is used in a variety of clinical settings in hospitals and in primary care, and the test is standard practice with the highest risk, critically ill patients.
ECG monitoring essentially falls in to two categories: 12-lead ECG recording and ECG rhythm monitoring. As the terms imply, the latter is used to monitor the heart's rhythm and identify any deviations from normal sinus rhythm, while the former is used primarily to ‘visualise’ anatomical surfaces of the heart to aid diagnosis of conditions such as myocardial infarction.
It is possible to record ECG rhythm without having to apply monitoring electrodes and cables, for example when using the AliveCor Kardia Mobile device, but they are required for continuous ECG monitoring in clinical settings.
In terms of quality assurance, ECG monitoring electrodes must meet the requirements of the American National Standards Institute and Association for the Advancement of Medical Instrumentation EC12:2000(R)2015 standard, which establishes minimum labelling, safety and performance requirements (SCST, 2017). The Society for Cardiological Science and Technology (SCST) does not make recommendations on electrodes, but also refers to the US standards.
ECG rhythm monitoring
In the clinical setting, monitoring a patient's ECG rhythm requires a minimum of three electrodes (Figure 1), which are connected to colour-coded leads to aid identification, and these are usually placed on the torso. However, it is also commonplace for five electrodes to be used (Figure 2), with four placed on the torso, one each near the corresponding limb, and one at the fourth intercostal space at the right sternal border. A five-lead system allows additional leads to be monitored, which this may be advantageous in certain clinical situations. Training courses for ECG rhythm recording and 12-lead ECG recording are available from Charles Bloe Training Ltd (www.cb-training.com).
 Figure 1. Three-lead system used in ECG rhythm monitoring
Figure 1. Three-lead system used in ECG rhythm monitoring  Figure 2. Five-lead system used in ECG rhythm monitoring
Figure 2. Five-lead system used in ECG rhythm monitoring
12-lead ECG recording
Recording a 12-lead ECG requires the application of 10 electrodes, one to each of the four limbs and six across the chest. The application of 10 electrodes (four limb electrodes and six chest electrodes) yields 12 leads—the information recorded by the 10 electrodes is combined to obtain 12 traces of the heart's electrical activity, hence the description of 12-lead ECG (Figure 3 and Figure 4).
 Figure 3. Twelve-lead ECG, with four limb and six chest electrodes
Figure 3. Twelve-lead ECG, with four limb and six chest electrodes 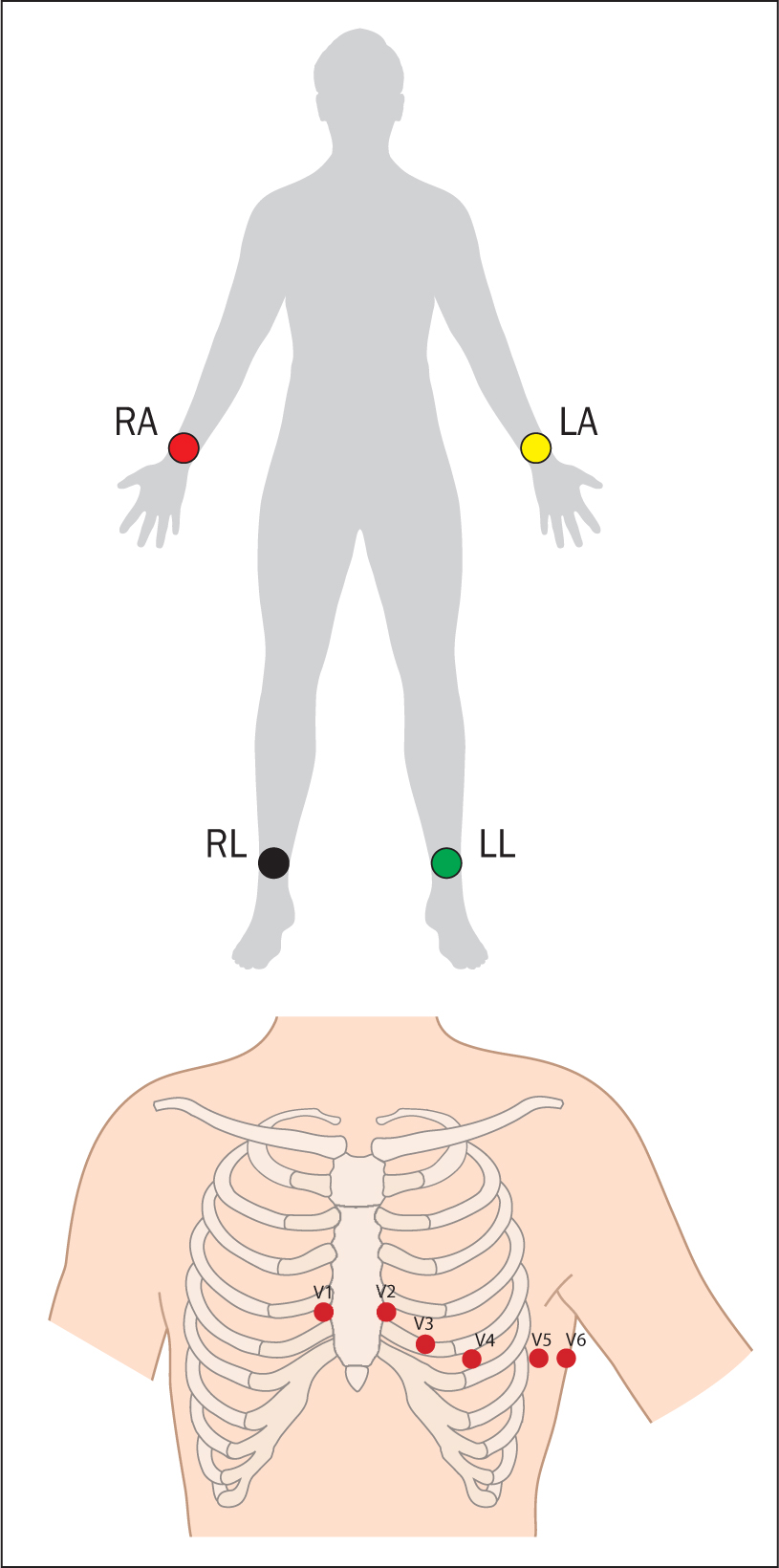 Figure 4. 12-lead ECG, with the positioning of four limb and six chest electrodes
Figure 4. 12-lead ECG, with the positioning of four limb and six chest electrodes
The limb leads visualise the heart in a frontal (coronal) plane. The chest leads in a horizontal (transverse) plane. Collectively, they view the key inferior, anterior and lateral anatomical surfaces of the left ventricle.
ECGs and infection risk
Healthcare-associated infections (HCAIs), or infections acquired in healthcare settings, are associated with high mortality and morbidity rates (World Health Organization (WHO), 2011). They are the most frequent adverse clinical event in healthcare provision. The term HCAI covers a wide range of infections, with the most well known including those caused by meticillin-resistant Staphylococcus aureus (MRSA), Clostridium difficile and Escherichia coli.
HCAIs are significant not only in terms of morbidity and mortality, but also in terms of the consequent high economic impact (Hollenbeak et al, 2000). Approximately 300 000 patients a year in England contract an HCAI (National Institute for Clinical Excellence (NICE), 2014) and the financial implications of this are considerable, with the NHS sustaining an estimated £1 billion in costs per year (NICE, 2017). Infection prevention and control is therefore a key priority for the health service (NICE, 2017).
The presence of bacteria on ECG cables and clips is common and more than half of the bacteria species found pose a risk or a potential risk for infection (Albert et al, 2010). Thorough cleaning of reusable ECG monitoring cables is difficult because of the multiple surfaces and intricacies of the equipment. Cleaning should only be carried out using non-bleach based cleaning wipes, otherwise the wires deteriorate. Even after cleaning, the presence of bacterial and fungal species on reusable ECG lead wires carries the risk of cross-contamination between patients, thereby increasing the risk of HCAI transmission. Pathogens could consequently be dispersed to high-risk patients, such as burns patients, those who are just out of surgery and those with open wounds. For example, research has linked a 21-patient vancomycin-resistant enterococcus (VRE) outbreak in a burns intensive care unit to microbial growth on reusable ECG lead wires (Falk et al, 2000; Brown, 2011).
Because electrocardiography wires cannot be sufficiently disinfected, they can contribute to the growth of resistant bacteria. The many pathways provided by reusable wires for cross-contamination with resistant bacteria increase the risk of HCAI. Cleaning practices for ECG leads, BP cuffs and pulse oximetry probes tend to be variable and inconsistent, ranging from no cleaning to the use of general detergent and antibacterial universal wipes.
Disposable ECG leads reduce risk of infection through these pathways. Adoption of disposable ECG leads as part of an overall infection control programme can decrease infection rates in acute healthcare facilities. The Kendall DLTM ECG Cable and Lead Wire System is single patient use and offers a reliable alternative to reusable leads with an added potential benefit of helping reduce HCAIs.
A number of reusable monitoring devices are employed in a range of healthcare settings. These include ECG monitoring cables, BP cuffs and pulse oximetry finger probes. However, there are no national guidelines on the decontamination and disinfection of these devices to reduce potential cross-infection.
Surgical site infection
The most common cardiac operations performed in the UK are coronary artery bypass grafting (CABG), followed by aortic valve replacement (AVR). Although the number of cardiac operations being performed in the UK has been steadily falling for more than a decade, upwards of 34 000 are still carried out each year (National Institute for Cardiovascular Outcomes Research, 2020). Most CABG and AVR procedures are performed through an open median sternotomy, although transcatheter aortic valve implantation (TAVI) may be undertaken percutaneously. Postoperatively, these patients are transferred to a specialist critical care unit and continuous cardiac monitoring is required.
Surgical site infections complicating CABG procedures are significant in terms of morbidity, mortality and economic impact (Hollenbeak et al, 2000; Brandt et al, 2020). Reusable ECG wires and cables, which are placed on the chest of a CABG patient close to the sternotomy incision, are often inadequately cleaned (Lestari et al, 2013)—they have been traced to vancomycin-resistant enterococci VRE outbreaks (Falk et al, 2000) and may pose a potential source of cross-contamination and surgical site incision pathogen transmission (Albert et al, 2010).
The Kendall DL single-patient-use ECG cable and wire system helps reduce the risk of cross-contamination between patients because it is used just once. Compared with reusable ECG lead-wire systems, the Kendall DL has been shown to lead to an average 14.3% reduction in estimated surgical site infection during the index admission, an 18% reduction at 30 days, a 21% reduction at 60 days, and a statistically significant 25% reduction at 90 days after CABG (P=0.04) (Lankiewicz, 2018). Transitioning to the Kendall DL single-patient-use ECG cable and lead wire system as part of a multimodal infection prevention strategy may therefore significantly reduce surgical site infection.
COVID-19
In late 2019, a new severe acute respiratory syndrome coronavirus (SARS-CoV-2) was identified in China, with the WHO designating COVID-19 as the name of the disease caused by the novel coronavirus on 11 February 2020, declaring the spread of the disease a global pandemic one month later (WHO, 2020).
Even before the WHO declared the pandemic, there were already major implications for the NHS, with an excess of hospital admissions seldom witnessed before as a result of COVID-19. By January 2021, more than 100 000 people in the UK had died within 28 days of a diagnosis of COVID-19 (Office for National Statistics, 2021). The pandemic occurred against the backdrop of a healthcare system that was already under strain. There were around 44 000 full-time equivalent advertised vacancies in hospital and community services in England alone between October and December 2019. This equates to an estimated shortfall of 12.1% (Royal College of Nursing (RCN), 2019a). Therefore, even before COVID-19, resources within the NHS were stretched.
A major survey carried out by the RCN in 2019 found that 61% of nursing staff said they were too busy to provide patients with the level of care they would like—a significant increase from 43% 10 years previously. More than half (54%) said they spent too much of their time on non-nursing tasks such as paperwork and general cleaning (RCN, 2019b). It would be reasonable to conclude that those pressures have increased since the start of the COVID-19 pandemic. Terminal cleaning of bed spaces and reusable equipment by nurses only adds to the non-clinical workload. There is a misconception that cleaning of equipment is done exclusively by healthcare support workers whereas, in practice, these tasks are often undertaken by nurses.
Against the backdrop of the COVID-19 pandemic, single-use devices, such as Kendall DL single-patient-use ECG wire system may help to prevent the risk of cross-contamination. With the pandemic putting additional pressures on the NHS workforce, single-use devices can also help free nursing time that would otherwise be taken up with cleaning equipment before use with the next patient.
Reduction in false alarms
Another benefit of using single-patient electrodes over reusable ECG electrodes relates to alarm events. Cardiac monitor alarm parameters are set to alert staff to adverse clinical situations and cardiac arrhythmias. Alarms may be categorised from advisory, such as a disconnected wire or minor interference, to lethal, for example a cardiac arrest rhythm.
Alarm fatigue in cardiac monitoring occurs when staff become desensitised to alarms when they repeatedly sound in error. However, although most of these warnings will be erroneous, the danger is that true alarms could be ignored, with catastrophic consequences (Keller, 2021). When taking time to respond to false alarms, nurses shift responsibilities away from the true needs of patients.
In a cluster randomised controlled trial of 1 611 patients having cardiac surgery in the USA, Kendall DL single-patient-use ECG electrode wires were shown to result in a 29% reduction in no-telemetry, leads-fail and leads-off alarms (RR=0.71, 95% CI 0.53 to 0.96) during a 4-month period. It also showed statistical non-inferiority in monitoring alarms and false alarms (P=0.002) (Lankiewicz et al, 2018). The reduction in false alarms may play an important role in patient safety by reducing ECG alarm fatigue.
Case study 1. CABG
David Thompson is a 49-year-old man. He has longstanding, poorly controlled diabetes and had a renal transplant 3 years ago. He was admitted 16 days previously with central chest pain and was diagnosed with a non-ST elevation myocardial infarction.
Coronary angiography demonstrated severe triple vessel coronary artery disease that was not amenable to percutaneous coronary intervention (PCI). He underwent inpatient triple vessel CABG and was discharged 7 days later.
He was readmitted 5 weeks later with recurrence of central chest pain and a further marginal rise in high-sensitivity troponin. He was managed in the coronary care unit with a suspicion of acute coronary syndrome. He had clear infection control challenges with poor glycaemic control, anti-rejection drugs and a recent sternotomy wound. Cardiac monitoring was essential in his situation because of the high risk of lethal cardiac arrhythmias.
It would be reasonable to consider single-use ECG monitoring leads in his situation given the challenges in balancing the requirement for good-quality ECG monitoring against a backdrop of recent surgical incision and high infection risk. Against that backdrop, it was decided to monitor Mr Thompson's ECG using Kendall DL single-patient-use ECG lead wires.
Case study 2. Transcatheter aortic valve implantation
Dorothy Martin is an 87-year-old woman who was admitted with increasing shortness of breath resulting from worsening aortic stenosis. She has mild cognitive impairment.
Urgent aortic valve replacement was considered necessary and, following a multidisciplinary team meeting, it was felt that transcatheter aortic valve implantation was preferable to conventional surgical aortic valve replacement. This was carried out the following week and she was stable throughout the procedure, although she was more confused postoperatively. She was managed in a medical high-dependency unit where cardiac monitoring was started.
Although significantly older than the previous patient, Ms Martin appeared to have a lower risk of infection control challenges. Continuous cardiac monitoring was desirable and was commenced using the Kendall DL single-use ECG electrode wires. However, given her confusion, she was not fully compliant, often trying to remove her monitoring electrodes. The Kendall DL single-use ECG lead wires include a patented clip, which can help with non-compliant patients. It can not be pulled off; therefore, patients have more effective recordings.
Case study 3. COVID myocarditis
Alice Fraser is a 79-year-old woman with multiple comorbidities, which include hypertension, diabetes, ischaemic heart disease, chronic obstructive pulmonary disease and mild cognitive impairment. She lives in a nursing home and has just tested positive for COVID-19 and was admitted with shortness of breath.
She was in need of level 2 care and was transferred to a high-dependency unit for management. Ms Fraser became dependent on high-flow oxygen and developed a COVID-related myocarditis, resulting in a number of significant atrial and ventricular cardiac arrhythmias; she therefore required continuous ECG rhythm monitoring.
Although Ms Fraser did not have an open wound, she was at increased risk of contracting an HCAI because of her multiple comorbidities and recent diagnosis. Because Kendall DL single-patient-use ECG electrode wires do not need to be cleaned in order to be used on another patient, they may help to reduce the risk of cross contamination between patients and health professionals. Therefore, as part of an overall infection reduction strategy, Ms Fraser was monitored using Kendall DL single-patient-use ECG wire system.
Conclusion
HCAIs result in significant patient harm and are expensive for healthcare providers. They are associated with increased lengths of stay and readmissions, yet many are preventable.
ECG monitoring is performed in a wide range of clinical areas, especially for patients who are undergoing surgery and the sickest and most vulnerable patients in critical care, and reusable ECG electrodes and cables can harbour microorganisms that are implicated in HCAIs. The use of the Kendall DL single-patient-use ECG cable and lead wire system as part of a multimodal infection prevention strategy may therefore serve to significantly reduce the risk of HCAIs. Although no single intervention can eradicate HCAIs, removing known cross-contamination vectors between patients must be considered.
This article has highlighted the considerable pressures that health professionals are already under that will undoubtedly have been exacerbated during the COVID-19 pandemic. Quite apart from the clinical benefits gained from reducing the risk of HCAIs, single-use monitoring cables avoid the need for terminal cleaning and thereby further reduce demands of healthcare professionals' time.
KEY POINTS
- The Kendall DL single-patient-use ECG cable and lead wire system has the potential to significantly reduce healthcare-associated infections (HCAIs) and postoperative surgical site infections
- Reducing HCAIs is a key focus for the NHS because this will reduce hospital stay and readmissions because of recurring infections
- Nurses are often responsible for terminal cleaning of equipment, such as reusable ECG leads, which takes them away from delivering direct patient care
CPD reflective questions
- What mechanisms are used to assess your patients risk of HCAIs?
- Are there any features of your clinical settings or common interventions that increase the risk of HCAIs?
- What are the main barriers to using single use clinical items in your area?