

Chronic diseases not only threaten the quality of life but also impose a significant burden on the economy in terms of health expenditure (Ünal et al, 2013). These diseases are also seen to have slow progression and a long duration. Alzheimer's disease is an irreversible brain disorder that is slow progressing and leads to memory loss and deteriorating thinking skills over a long period of time (Leung et al, 2018). According to recent evidence, vitamin D is associated not only with its known effects on calcium and bone metabolism but also with many chronic diseases due to the widespread presence of vitamin D receptors in the body (Staud, 2005; Mpandzou et al, 2016; Veldurthy et al, 2016). In addition, inadequate vitamin D intake with ageing has been reported and vitamin D deficiency is presumed to be associated with Alzheimer's disease (Meehan and Penckofer, 2014). Vitamin D is sometimes referred to as the ‘sunshine vitamin’ since it is synthesised in humans when the skin is exposed to ultraviolet-B (UVB) light from the sun, as well as being obtained from dietary sources, and both routes are important in maintaining optimum levels (Nair and Maseeh, 2012). Reduced outdoor activities, skin wrinkles or poor skin integrity and malabsorption disorders with ageing are held responsible for low vitamin D in patients with Alzheimer's disease (Meehan and Penckofer, 2014).
In the context of vitamin classifications, scientists have concluded that vitamin D usually acts as a hormone rather than a vitamin (Reichrath et al, 2007; Nair and Maseeh, 2012). Vitamin D in the nervous system participates in calcium-mediated neuronal activities and neurotransmitter metabolism (Banerjee et al, 2015). The aim of this article was to carry out and report on a thorough literature review on the potential benefit of vitamin D supplementation in individuals with Alzheimer's disease living in the community and to identify implications for practice and further research.
Background
Increased age may result in significant changes, such as the accumulation of harmful substances and the lack of essential vitamins and minerals in the body (Fusco et al, 2007; Rahal et al, 2014). Alzheimer's disease primarily manifests itself with cognitive impairment. According to Kurella Tamura and Yaffe (2011), patients with cognitive impairment and dementia have a higher risk of death. In a systematic review and meta-analysis, Balion et al (2012) showed that individuals with Alzheimer's disease had lower 25-hydroxyvitamin D concentrations (also referred to as 25(OH)D) compared with those without Alzheimer's disease. Furthermore, more recent research has provided evidence that vitamin D has a positive effect on many chronic diseases.
However, detrimental effects of vitamin D have also been reported. Alshahrani and Aljohani (2013) indicated that serum vitamin D levels (in the form of 25-hydroxyvitamin D) have a level of toxicity (over 150 ng/ml), which occurs after consumption of 40 000 IU/day. Thus, excessive increases may lead to different side-effects and deterioration of health. Hypercalcaemia caused by vitamin D toxicity is held responsible for symptoms including irregular heartbeat, muscle pain and kidney stones. Schlögl and Holick (2014) suggested an association between vitamin D and many chronic diseases, including neurocognitive failure (Buell and Dawson-Hughes, 2008; Balion et al, 2012).
Furthermore, vitamin D receptors have been found in more than 200 genes and 37 different tissues, including the brain (Carlberg and Campbell, 2013). Although the presence of a vitamin D receptor in the brain is known, the role of vitamin D and how it works in the brain remains unclear (Girgis et al, 2014; Pike, 2014). A deeper understanding of this process may help determine whether vitamin D supplementation has an impact on the maintenance of cognitive function in patients with Alzheimer's disease.
The role of vitamin D in the nervous system
To put this review in context, the results of recent research trying to explain the presence of vitamin D in the nervous system need to be synthesised briefly. Latimer et al (2014) studied synaptic functions in animals to explain the role of vitamin D in the nervous system and concluded that the important role of the contactin complex in anchoring myelin to the axons was provided by vitamin D-mediated processes. In addition, the basis of neuronal communication is dependent on nerve conduction provided through axons and insulated by myelin, a fatty white substance, which needs vitamin D to be anchored to the axon (Latimer et al, 2014) (see Figure 1). The model indicates that the human brain may be affected by the lack of vitamin D.
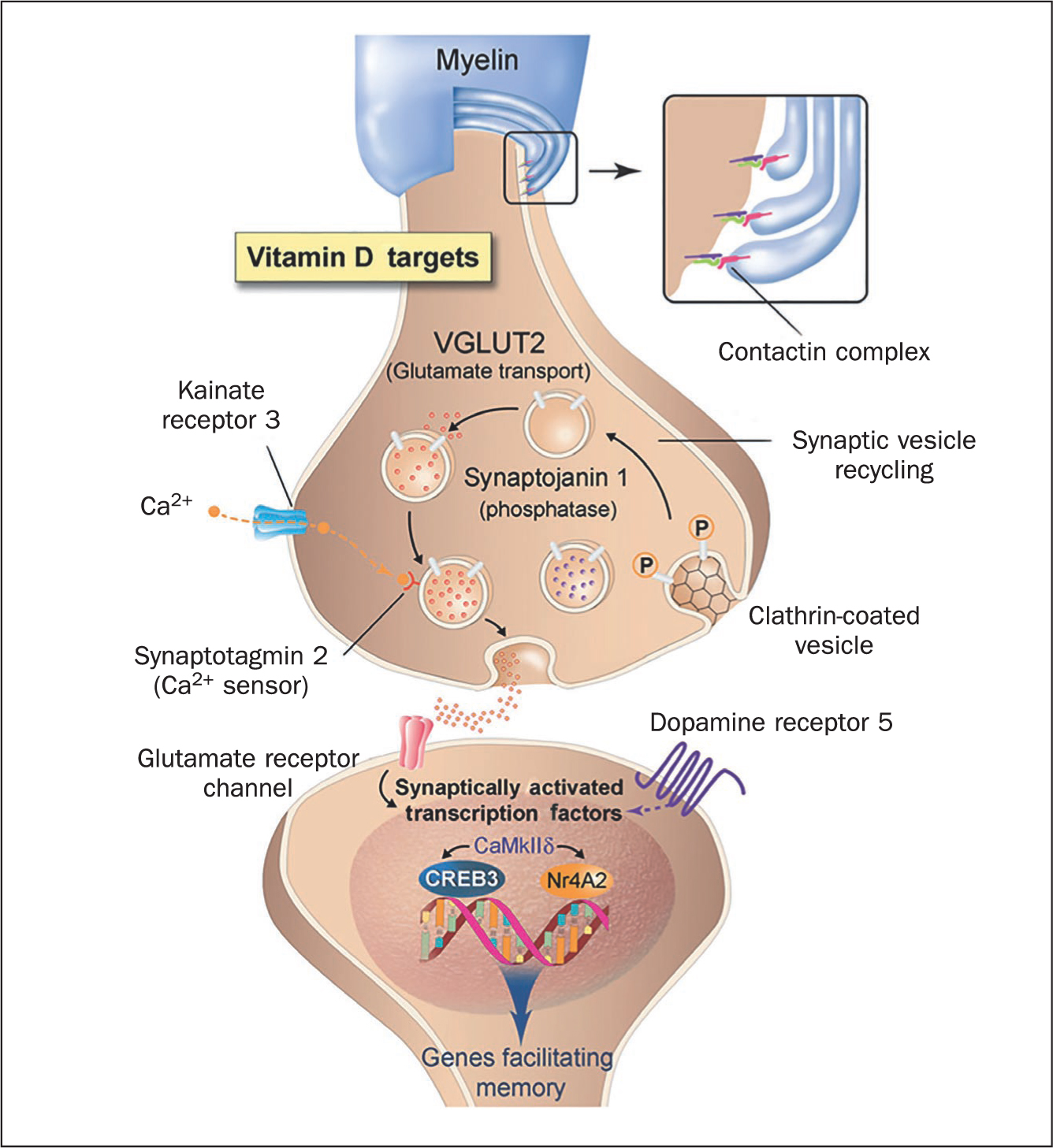
Further evidence supporting Latimer et al may lie in the findings of Landel et al (2016), who tried to explain the complexity of vitamin D-mediated processes in Alzheimer's disease in compliance with another well-known effect of vitamin D, relating to neurotransmitter release. They defined new mechanisms to explain the role of vitamin D-mediated processes in Alzheimer's disease, including oxidative stress, inflammatory processes and neurotransmission, which need optimum levels of vitamin D (Box 1). Littlejohns et al (2014) emphasised that in vitro axon degeneration models in cell cultures induced by β-amyloid peptide and glutamate showed a significant recovery after vitamin D supplementation. Moreover, phagocytic clearance of amyloid plaques was increased by the presence of vitamin D in culture dishes of tissue samples taken from patients diagnosed with Alzheimer's. The absence of vitamin D, as first demonstrated by Eyles et al (2003) and verified by Gezen-Ak et al (2007), results in decreased levels of nerve growth factor, which means that optimum-level vitamin D is essential for mental health. Finally, optimum vitamin D levels are crucial for proper vascular processes, neurotransmission, protein accumulation, oxidative stress, inflammation and the immune system (Landel et al, 2016).
Box 1.Vitamin D-mediated processes in Alzheimer's diseaseVitamin D imbalance affects the following:
- Vascular processes
- Calcium homeostasis
- Neurotransmission
- Oxidative stress
- Inflammation and immune system
- β-amyloid and tau protein accumulation
Source: Landel et al, 2016
Researchers have focused on whether vitamin D has an impact on the nervous system both in human and animal studies, as well as in vitro models. All models provided valid results but the work of Landel et al (2016) is noteworthy because it also indicates that the effects of vitamin D on mental health are multifactorial and depend on genetic, immune-mediated, environmental, nutritional and hormonal factors. Cultural factors are also significant on maintaining vitamin D levels. For example, the style of dress common in Muslim societies where even the face is veiled is held responsible for low vitamin D levels in women. Overall, all authors have proposed a role for vitamin D in mental health, but the exact mechanisms of action are still unclear.
People living in the community with Alzheimer's disease
Alzheimer's disease primarily manifests with cognitive impairment and it is known as the most common type of dementia (Karantzoulis and Galvin, 2011). According to the World Alzheimer Report 2016, more than 47 million people live with dementia across the world, and it has been estimated that the number will increase up to 131 million by 2050 (Prince et al, 2016). Lepore et al (2017) reported that only one-fifth of people with Alzheimer's and dementia live in residential care settings or nursing homes. Most people with Alzheimer's disease live in the community but are often dependent on others for their day-to-day care.
The proportion of people living alone is approximately 30% and it is higher than those living in residential care settings or nursing homes (Lepore et al, 2017). Caregivers are often family members or spouses who need to provide on average 24.4 hours of care per week and have difficulty in performing nursing duties (National Alliance for Caregiving and AARP Public Policy Institute, 2015). The difficulty in carrying out nursing tasks stems from the fact that caregivers are more likely to have other caring roles; approximately one-third of caregivers are over 65 years old, and one-quarter is defined as ‘sandwich’ carers, with care responsibilities for both parents and children under 18 years old (Lepore et al, 2017). The burden of dealing with Alzheimer's and dementia can be greater than expected because it has both a financial and an emotional impact on the family. The Alzheimer's Association (2014) found that approximately 10% of caregivers had quit their jobs and 13% of caregivers had switched from full-time jobs to part-time work.
For people living in the community with Alzheimer's disease, both pharmacological and non-pharmacological interventions may reduce the burden of disease. Vitamin D supplementation might be useful because it is a pharmacological method that is cheap, practical and easy to apply at home by both caregivers and patients. The benefits and potential risks of vitamin D supplementation may be demonstrated only by long-term studies. If the potential benefits of vitamin D supplementation in patients with Alzheimer's disease were known, multifactorial risks associated with vitamin D involving oxidative stress, inflammatory processes and vascular processes could be better explained and eliminated. The current knowledge raises the possibility that improving vitamin D levels in people living with Alzheimer's disease could potentially improve their cognitive ability, patient outcomes and quality of life.
Formulating the question
Given the evidence cited above, vitamin D supplementation may have an impact on cognition and may be beneficial for people living with Alzheimer's disease. The rationale for this literature review was, therefore, to summarise and synthesise the existing evidence relating to any effect of vitamin D supplementation on cognition in the elderly in the community. The PICO tool (Lau, 2007) was used to formulate a research question (Table 1). This literature review is therefore driven by the following research question: Is vitamin D supplementation of potential benefit for community-living people with Alzheimer's disease?
Table 1. PICO sections in formulating research question
| Population | Patients with Alzheimer's disease in the community |
| Intervention/Indicator | Benefit of vitamin D supplementation |
| Comparison | Patients with Alzheimer's disease without supplementation |
| Outcome | Possible positive or negative outcomes on cognitive function |
Methodology
This review was designed to examine the existing knowledge base for the findings of intelligence tests, brain imaging, and blood and spinal fluid tests in relation to individuals' consumption of vitamin D supplementation in the community (Tangney et al, 2011). A literature review was chosen as a method enabling a review of the current state of the relevant science, a summary of the existing points, a new angle of view, and an evaluation of the applicability of theoretical foundations to the current practice (Aveyard, 2014). It was decided to study the assumed association by reviewing peer-reviewed scholarly articles citing evidence from intelligence tests, brain imaging, and blood and spinal fluid test results for people in the community exposed to vitamin D supplementation or not.
Electronic database search
PubMed, EMBASE, Cochrane Library and CINAHL were determined as the most appropriate data sources. The list of the developed search words included but was not limited to: ‘vitamin D’, ‘supplementation’, ‘Alzheimer's disease’, ‘cognitive functions’ and ‘mental health’. For instance, MeSH (Medical Subject Headings) terms were used to identify the relevant keywords for vitamin D. Search terms expanded as vitamin D deficiency, vitamin D receptors, cholecalciferol and ergocalciferols (Table 2).
Table 2. Search terms
| Vitamin D OR vitamin D supplementation OR vitamin D deficiency OR vitamin D receptors OR cholecalciferol/ergocalciferols | |
| AND | Alzheimer's disease/syndrome OR neurocognitive disease/disorders OR neurodegenerative disease/disorder OR memory impairment |
| AND | Memory facilitation OR improved neuronal communication OR neurotransmission |
Inclusion criteria
The keyword-based search through the four selected databases was highly productive and resulted in a large volume of peer-reviewed articles being obtained. These were subject to further refinement to remove duplicates and the rest were analysed in compliance with the formulated inclusion criteria:
- Publication date (the period between 2011 and 2018)
- Access to full copy of paper
- Papers with a focused research question evaluating individuals' cognitive abilities with intellectual tests, brain imaging or use of blood and spinal fluid tests, and consumption of vitamin D supplementation
- English language publication.
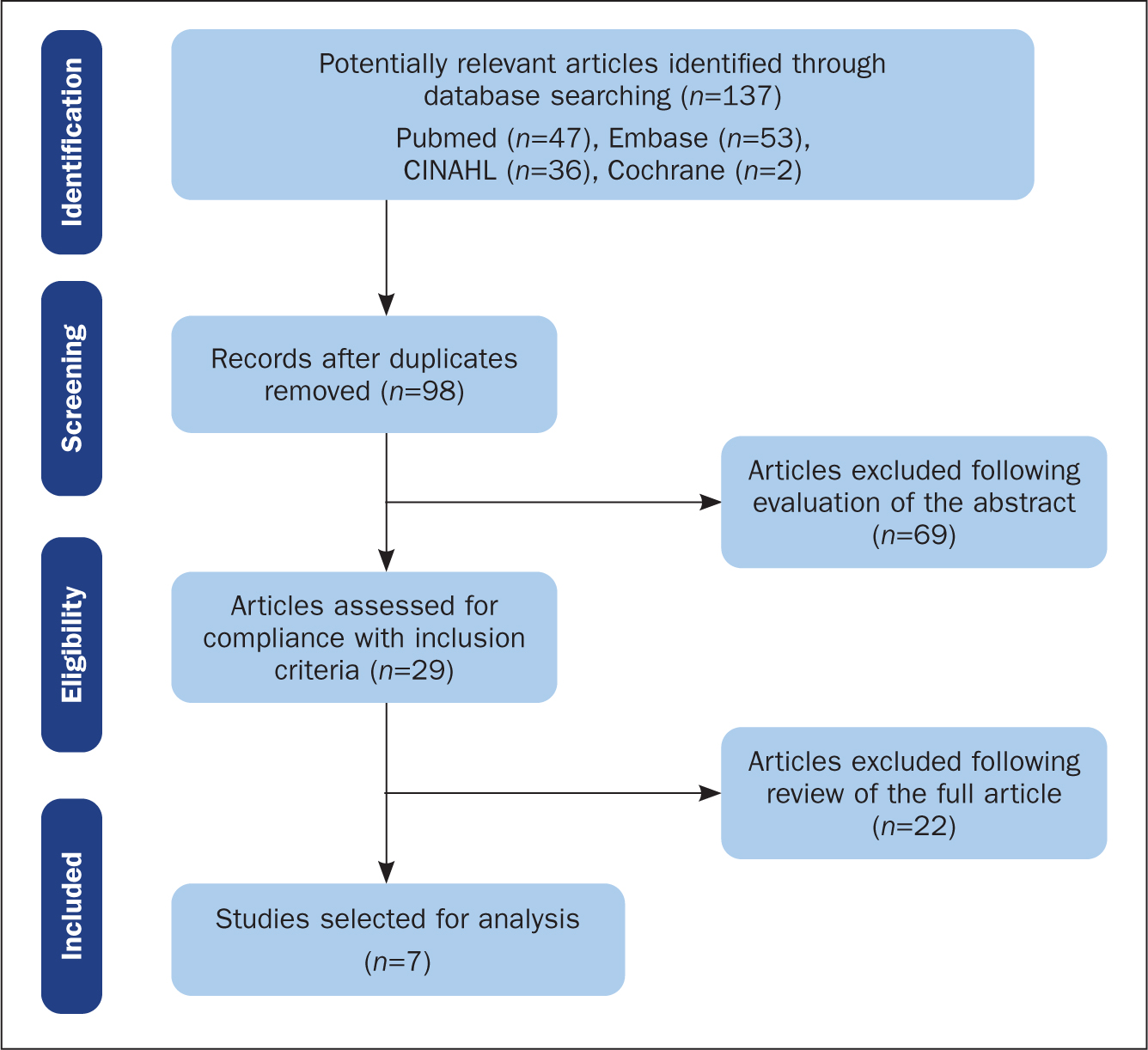
Correspondingly, studies published in a language other than English, or addressing the issue of Alzheimer's disease without any reference to cognition measurement tools, and case reports/conference papers were excluded. Potentially relevant articles were further reviewed by reference to the abstract and the full content in order to define a final set for analysis and to avoid bias (Figure 2).
Critique tools
The toolkit developed by the Critical Appraisal Skills Programme (CASP) (2022) is commonly used for critically appraising the literature chosen for a systematic review. The CASP toolkit offers different checklists to evaluate the quality of randomised controlled trials, case-control studies, cohort studies, systematic reviews and other academic endeavours. The use of the developed search strategy contributed to a non-biased and transparent manner of selection of articles, and the CASP checklists ensured the researcher's objectivity in evaluating the credibility and quality of the selected papers.
Investigations of variables and outcomes
The available scope of cognitive assessment tools is divided into three categories: intellectual tests, brain imaging, and blood and spinal fluid testing (Rosli et al, 2016). In practice, these tests are also classified as invasive and non-invasive. The use of invasive procedures in patients with Alzheimer's requires special ethical considerations. However, no ethical principles regarding patient safety were stated for any study. Littlejohns et al (2014), Granic et al (2015), Miller et al (2015) and Hooshmand et al (2014) reported only obtaining ethical approval from an institutional review board. The Mini-Mental State Examination (MMSE), which was first developed in 1975 by Folstein et al, is one of the most frequently used tools in clinical practice to assess cognitive impairment (Sugarman and Axelrod, 2014). Therefore, MMSE scores and vitamin D levels were taken into account with studies assessing cognitive impairment.
Brain imaging, an alternative to intellectual tests, is a useful method for diagnosing cognitive impairments or revealing changes in the brain (Pan et al, 2013). Research in this field has identified the role of proteins – tau protein and β-amyloid – in reducing neurological function (Jin, 2015). A decreased mass of cerebral cortex and dead nerve cells surrounded by β-amyloid protein are primary symptoms of declining cognition. Therefore, monitoring visible changes in the brain allows the identification of affected areas, which is critical for cognitive assessment and diagnosis (Jin, 2015). The study conducted by Hooshmand et al (2014) revealed a relationship between higher 25-hydroxyvitamin D levels and larger brain volumes, as well as for white matter and temporal lobe. These findings are taken into account for the distribution of vitamin D receptors in the brain. It has, therefore, been suggested that decreased temporal lobe function alongside low vitamin D exposure may be related to speech problems, impaired memory and hearing loss in Alzheimer's patients.
Finally, the findings of blood and spinal fluid tests may indicate early signs of neurodegenerative diseases (Forlenza et al, 2015). A study conducted by Bredesen (2015) showed that the nature of and disparity in the underlying processes of different forms of cognitive impairment could be monitored and observed through plasma and spinal fluid sampling (Swan and Evans, 2022). The relationship between the β-amyloid levels in cerebrospinal fluid and serum vitamin D levels was considered when reviewing the studies. Given the efficiency of these three approaches to cognitive assessment, this literature review paid particular attention to the measurement tool used when investigating the potential benefit of vitamin D for cognitive function.
Results and discussion
The comprehensive screening process resulted in the selection of seven peer-reviewed journal articles: one was a clinical trial, five were cohort studies and one was a systematic review (Table 3). All of them were thoroughly evaluated regarding quality using the CASP (2022) critical appraisal tools for randomised-controlled trials, cohort studies and systematic reviews. Except for some points, all reviewed studies produced credible findings by following academic guidelines for problem development, research methods, participant sampling and selection, research procedures, outcomes measurement, and reporting.
Table 3. Articles selected for review
| Author(s) and year | Title |
|---|---|
| Aspell et al (2017) | Effects of vitamin D supplementation on cognitive function in healthy, community-dwelling older adults: Results from a randomized double-blind placebo-controlled pilot trial |
| Granic et al (2015) | Serum 25-hydroxyvitamin D and cognitive decline in the very old: The Newcastle 85+ study |
| Hooshmand et al (2014) | Vitamin D in relation to cognitive impairment, cerebrospinal fluid biomarkers, and brain volumes |
| Littlejohns et al (2014) | Vitamin D and the risk of dementia and Alzheimer disease |
| Miller et al (2015) | Vitamin D status and rates of cognitive decline in a multi ethnic cohort of older adults |
| Tofanello et al (2014) | Vitamin D deficiency predicts cognitive decline in older men and women |
| Annweiler et al (2013) | Low serum vitamin D concentrations in Alzheimer's disease: A systematic review and meta-analysis |
However, it was challenging to limit the literature review research specifically to Alzheimer's disease because most primary research studies have examined the role of vitamin D in cognitive performance in relation to several cognition-related illnesses characteristic for the elderly, namely in community dwelling healthy older adults, Alzheimer's disease, dementia and mild cognitive impairment. It is important to note that the population of the clinical pilot trial carried out by Aspell et al (2017) was community-dwelling healthy older adults. It was included as the most up-to-date study at the time of the search, and the pilot study may have parallel results with the following cohort studies and randomised controlled trials. In addition, Aspell et al (2017) did not confirm a positive association between vitamin D concentrations and cognitive function in older adults, whereas the cohort studies of Tofanello et al (2014), Littlejohns et al (2014), Hooshmand et al (2014), Miller et al (2015) and Granic et al (2015), along with the systematic review by Annweiler et al (2013), illustrated the prevalence of dementia, mild cognitive impairment and Alzheimer's disease among older people with low 25-hydroxyvitamin D levels.
Except for the systematic review (Annweiler et al, 2013), all of the included studies used intellectual test scores to measure individuals' global cognitive function, attention, and executive cognition. The use of blood tests to measure vitamin D levels was also a widespread practice. This method is indispensable for determining the serum level of vitamin D but, in the near future, it may be replaced by forms of measurement of vitamin D that can assist with making a differential diagnosis, such as measurement of levels of only skin-derived or only dietary intake of vitamin D.
Furthermore, Hooshmand et al (2014) assessed cognition through cerebrospinal fluid biomarkers and brain volumes, and concluded that there was a significant reduction of brain mass in patient with Alzheimer's disease. In addition, an in-depth analysis of these data may suggest that the reduction in brain mass not only leads to a decrease in cognition but also decreases the quality of life. Overall, the literature review revealed the prevalence of Alzheimer's disease, dementia and mild cognitive impairment in the elderly related to vitamin D deficiency or insufficiency. However, none of the reviewed studies provided evidence of a positive impact of vitamin D supplementation on cognitive function in the elderly with Alzheimer's disease or dementia, and this requires further discussion of the literature review findings.
Vitamin D and cognitive functions
The findings of Latimer et al (2014), Schlögl and Holick (2014) and others suggested a linear association between vitamin D deficiency and delayed cognition in patients diagnosed with dementia and Alzheimer's disease. The role of vitamin D in the vascular processes, β-amyloid and tau protein accumulation, neurotransmission, and inflammation and the immune system, suggested the idea that the natural decline in vitamin D levels may contribute to the development of Alzheimer's disease (Landel et al, 2016). In this respect, it was assumed that vitamin D supplementation is likely to maintain and sustain cognitive function in people diagnosed with Alzheimer's disease. However, the reviewed studies did not prove this point.
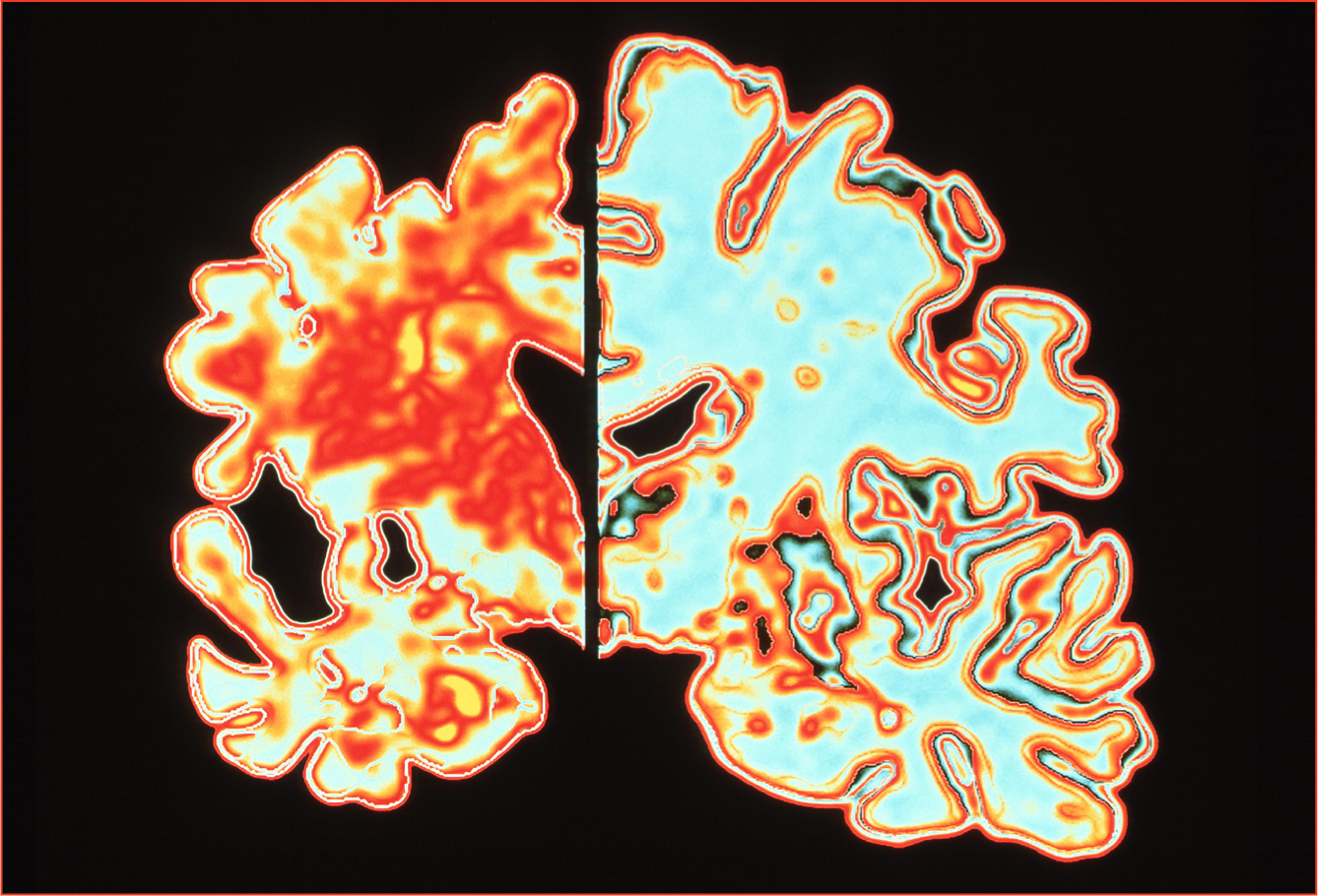
Orally administered supplements may not be absorbed well enough from the intestine with ageing or there may be a deficiency in the amount of skin-derived form of vitamin D with ageing. Therefore, a more focused research question is required for understanding of vitamin D-related aspects of Alzheimer's disease, for example to distinguish between insufficient skin-derived and inadequate dietary intake of vitamin D. More precisely, Annweiler et al (2013), Littlejohns et al (2014), Tofanello et al (2014) and Miller et al (2015) illustrated the prevalence of vitamin D deficiency in Alzheimer's disease cases by comparing 25-hydroxyvitamin D in blood samples and intellectual test scores, but the mechanism of causation is still unclear. Hooshmand et al (2014) measured the association between vitamin D and cognition through the coincidence of low 25-hydroxyvitamin D levels and lower brain volumes and abnormal proteins. In the context of the relationship between Alzheimer's and the mass of the cerebral cortex (Jin, 2015) (Figure 3), the findings of Hooshmand et al (2014) may contribute to the assumed association between vitamin D levels and cognitive function. At the same time, the cohort study by Granic et al (2015), which was based on a Standardized Mini-Mental State Examination (SSME), assessment of global cognitive function and attention in compliance with 25-hydroxyvitamin D level, showed that excessive increase in vitamin D levels is associated with poor attention; they concluded that global cognitive functions are maintained at optimum levels, not at low or high 25-hydroxyvitamin D concentrations. These findings may raise questions about the benefits of vitamin D supplementation for improving cognition, but it should be noted that supplements may be beneficial at optimum dosage, bearing in mind that a vitamin D intake of over 150 ng/ml is considered toxic (Alshahrani and Aljohani, 2013).
In contrast, the pilot clinical trial undertaken by Aspell et al (2017) rejected a relationship between vitamin D levels and cognitive performance in the elderly. As mentioned, the findings of Aspell et al's (2017) pilot may have parallels with those of the other studies reviewed, but the reliability of the results depends on the feasibility, duration, cost and sample size of each study. The articles included in the review were evaluated for their quality in accordance with the CASP critical appraisal checklists. It is possible to conclude that the general view in literature does not justify prescribing vitamin D supplementation to individuals with Alzheimer's disease to improve their cognitive performance.
It has been widely reported that low 25-hydroxyvitamin D levels in Alzheimer's disease should be considered biomarkers for the disease. So far existing knowledge does not support a scientific position regarding a positive association between vitamin D scores and cognitive functions in Alzheimer's disease. There is, therefore, no clear rationale for prescribing vitamin D to sustain cognitive function. However, Annweiler et al (2013), Littlejohns et al (2014), Tofanello et al (2014), Hooshmand et al (2014) and Miller et al (2015) have stressed the association between vitamin D deficiency and lower attention. Lower attention in patients with Alzheimer's disease may potentially impact on quality of life regarding fulfilling their daily needs and being dependent on others. For instance, patients who could not maintain attention in order to cross a road would be reluctant to take part in outdoor activities and may have poor physical and mental health, meaning they would need to depend on assisted living arrangements. In highlighting the association between vitamin D deficiency and lower attention in older people, those studies could not identify a potential benefit for supplementing vitamin D intake in people with Alzheimer's disease in terms of improving memory and cognition.
Conclusions, limitations and implications for practice
This work has synthesised the current knowledge about the potential benefit of vitamin D supplementation in patients with Alzheimer's disease relating to their cognitive performance. The majority of studies have highlighted the role of vitamin D contributing to the neurocognitive processes in Alzheimer's disease, and suggested that optimum vitamin D levels are essential in maintaining cognition (Schlögl and Holick, 2014; Granic et al, 2015). Due to complex vitamin D-mediated processes in Alzheimer's disease, low vitamin D scores may be indirectly responsible for reduced quality of life (Landel et al, 2016). The majority of reviewed studies also stressed an association between vitamin D deficiency and lower attention (Annweiler et al, 2013; Granic et al, 2015; Aspell et al, 2017). However, the association between lower vitamin D scores and lower intellectual test scores does not imply the ability of vitamin D to sustain or increase cognitive function. Similarly, the relationship between vitamin D levels and brain volumes and cerebrospinal fluid biomarkers, do not guarantee the ability of vitamin D supplementation to sustain cognition (Hooshmand et al, 2014).
The studies were found to be of good quality by applying the CASP critical appraisal process; however, their findings are of more value for current research rather than clinical practice. In current practice, studies measuring 25-hydroxyvitamin D levels in blood tests are widely performed, but these do not identify which form of vitamin D is deficient. Theoretically, it is still unclear whether or not there is a conversion disorder due to skin wrinkles, impaired absorption from the gut or inadequate vitamin D intake with ageing. This is significant because understanding which form of vitamin D is missing and which way of administration is beneficial may allow us to choose the correct form and correct route of administration. The idea of distinguishing between insufficiency of skin-derived and dietary intake of vitamin D in older people may improve the understanding of which route of supplementation would be more useful in practice.
Due to the lack of consensus among the reviewed studies regarding supplementation with vitamin D in Alzheimer's disease, this literature review did not answer clearly any potential positive or negative outcomes on cognitive function. It is possible to conclude that, so far, low vitamin D levels can be interpreted only as early symptoms of dementia, mild cognitive impairment, and Alzheimer's disease (Balion et al, 2012). This literature review was limited by the secondary nature of the data and the scarcity of clinical trials addressing a potential benefit of vitamin D supplementation in sustaining cognitive function in Alzheimer's disease.
Limitations were mitigated in this current review by the use of the CASP appraisal tools to verify the quality and credibility of the selected sources of data. The most significant limitation of this research is revealing the relationship between vitamin D deficiency and lower attention in older people without providing an explanation of the exact mechanisms in the light of the current literature. Therefore, further research is needed to clarify vitamin D-related aspects of Alzheimer's disease.
The key recommendation for further studies would be to distinguish between insufficiency of skin-derived and dietary intake of vitamin D in older people in order to understand which route of supplementation is best for Alzheimer's patients in practice. While investigating the effects of skin-derived vitamin D in the elderly, studies should be carried out to allow individuals to take advantage of the sunlight on a regular basis.
KEY POINTS
- There is increasing interest in the link between vitamin D and chronic disease, and in particular on a possible role in cognitive function
- This literature review looked at whether vitamin D supplementation may have an impact on cognition and may be beneficial for people living with Alzheimer's disease
- The review concluded that, despite an association between vitamin D levels and lower attention in older people, there is no clear evidence of a positive benefit for supplementation in this group
- There is a need for further research to clarify the relationships, mechanisms and impact of vitamin D in people with dementia – which presents ethical issues for researchers
CPD reflective questions
- What factors might be responsible for low levels of vitamin D with ageing?
- Why might researchers want to find ways to distinguish between levels of skin-derived and food-absorbed forms of vitamin D?
- What are the detrimental effects of too much vitamin D?