

On 9 January 2020, the World Health Organization (WHO) reported a cluster of patients with pneumonia who were infected with a novel coronavirus (COVID-19) in Wuhan, China (WHO, 2020a). On 30 January the WHO declared the subsequent outbreak a public health emergency of international concern (WHO, 2020b). COVID-19's virulence and lethality meant that its effects were of a different order than the normal seasonal flu, to which it was often inappropriately compared. Many of those infected showed no or only mild symptoms, but, some individuals required intensive care treatment in hospital (Freedman, 2020).
In the UK, delivery of every aspect of care by all clinical and non-clinical departments needed reassessing and fundamentally reorganising in the expectation of an imminent surge of patients with COVID-19 during March 2020 (Stevens and Pritchard, 2020). On 23 March 2020, the UK government announced that people must remain at home except for essential purchases, work and travel, medical needs, one form of exercise per day, or providing care for others. All public gatherings and social events except funerals were prohibited and most retail businesses closed (Freedman, 2020). The government made sanctions for case isolation, social distancing and household quarantine to reduce the peak of the epidemic and the resulting pressure on NHS hospitals (Public Health England (PHE), 2020).
One of the most important tasks during the early part of the pandemic was the provision of capacity to support people with acute healthcare needs in hospitals by organising the safe and rapid discharge of those patients who were optimised for discharge (Willan et al, 2020). The COVID-19 Hospital Discharge Service Requirements (Department of Health and Social Care (DHSC), 2020) asked acute providers to rapidly update their processes and ways of working to deliver a discharge model that required staff to consider each patient in their unit and ask the questions: ‘Why not home? Why not today?’ One of the challenges for hospital clinical teams was deciding what management could be continued outside the hospital with community/district nurses, such as providing intravenous (IV) antibiotics.
Community intravenous therapy/outpatient parenteral antibiotic therapy
Early outpatient parenteral antibiotic therapy (OPAT) services in the UK were developed by a few clinical enthusiasts. These services have become widely recognised and, in turn, have been able to guide, educate and help other clinicians in the UK looking to set up OPAT services (Kayley, 2012).
OPAT provision has grown considerably over the past 10 years in the NHS and is now well-established in most UK regions (O'Hanlon et al, 2017). The benefits of community IV therapy are well-documented, and include cost savings (Gunderson et al, 2018), improved patient experience (Chapman et al, 2012), high levels of patient satisfaction (Al Alawi et al, 2015), provision of a safe and clinically competent service (Gray et al, 2012) and safe administration of treatment (Higginson, 2018).
There are two distinct cohorts of patients treated with OPAT; those who have IV therapy initiated in hospital and continued at home and those who can have treatment initiated and carried out exclusively in community settings (Nazarko, 2014).
Supporting hospital discharge: acute trust-initiated OPAT
OPAT in the UK has predominantly been delivered by teams based in acute hospitals. Such services tended to deliver OPAT through one or more of three models: the ‘infusion centre’ model, where patients attend an OPAT facility daily; the ‘visiting nurse’ model, where a nurse (from either primary or secondary care) delivers therapy in the patient's home; or the ‘self-administration’ model, where the patient or a carer is taught to administer therapy with regular supervision from the OPAT service (Chapman et al, 2019).
The challenge for health professionals is to enable people who are having OPAT to receive the best quality of care outside the traditional hospital environment; the success of this ambition will depend on community and acute staff breaking down barriers to provide truly integrated care (Nazarko, 2014).
Avoiding hospital admission/primary care-initiated OPAT
The recent growth of OPAT services based entirely in the community is a safe model of care, as long as the nurse administering therapy is trained and equipped to manage adverse reactions, including anaphylaxis (Chapman et al, 2012). Historically, the first and second doses of parenteral medication were administered in hospital due to the risk of an adverse reaction and it was advised that a hospital was the safest place for this procedure (Nathwani and Morrison, 2001). A randomised controlled trial (RCT) of home versus hospital-administered IV antibiotics indicated that IV antibiotic therapy administered in the home carries no greater risk than when administered in hospital (Wolter et al, 2004). There is no greater risk in administering the first and second doses of therapy in patients own homes and it is safe to do so (Trowbridge and Kralik, 2006).
A dedicated community IV therapy team can provide enhanced expertise in the management of different devices and antimicrobial agents and in practical skills such as venepuncture and cannulation. However, service capacity may be limited by a small team, particularly over large geographical areas. The use of the larger pool of community nurses provides greater capacity and also allows nurses to deliver more than one type of care to housebound patients at the same visit, for example wound or ulcer dressings and insulin injections. However, community nursing teams may, in an effort to manage their workload, restrict the number of OPAT patients they are able to support (Nazarko, 2014).
The service commissioned in the author's area—the boroughs of St Helens and Knowsley—has initiated treatment for patients needing IV therapy in a community setting since 2005. Initial service delivery was reliant on community nurses throughout the local boroughs, supported by two dedicated IV specialist nurses, competent in peripheral cannulation, midline and peripherally inserted central catheter (PICC) placement. The service expanded in 2012 driven by GP-led commissioning and the ever-growing need to manage patients outside of hospital. Figure 1 shows how referrals to the community IV therapy (CIVT) team has expanded. Additionally, four dedicated IV nurses were recruited to the CIVT team to meet increasing demand.
Figure 1. Annual referrals to the community IV therapy team
The team delivers medication across two boroughs between 7am and 10pm seven days a week. This enables patients on once-, twice- and three-times daily medication to be accepted on to the service the same day as they are optimised for discharge or referred in via primary care (capacity permitting). Patients with a permanent venous access device needing longer term therapy are supported by community nurses with ongoing support from the CIVT team to ensure there is always capacity within the service to accommodate new referrals with immediate effect. Nearly all therapy is delivered in the patient's home environment, with only a small number of patients attending a clinic setting to receive the IV antimicrobial therapy/long term venous access device placement. Figure 2 shows the various sources of referrals to the CIVT team before the pandemic. Figure 3 shows sources of referrals during the pandemic.
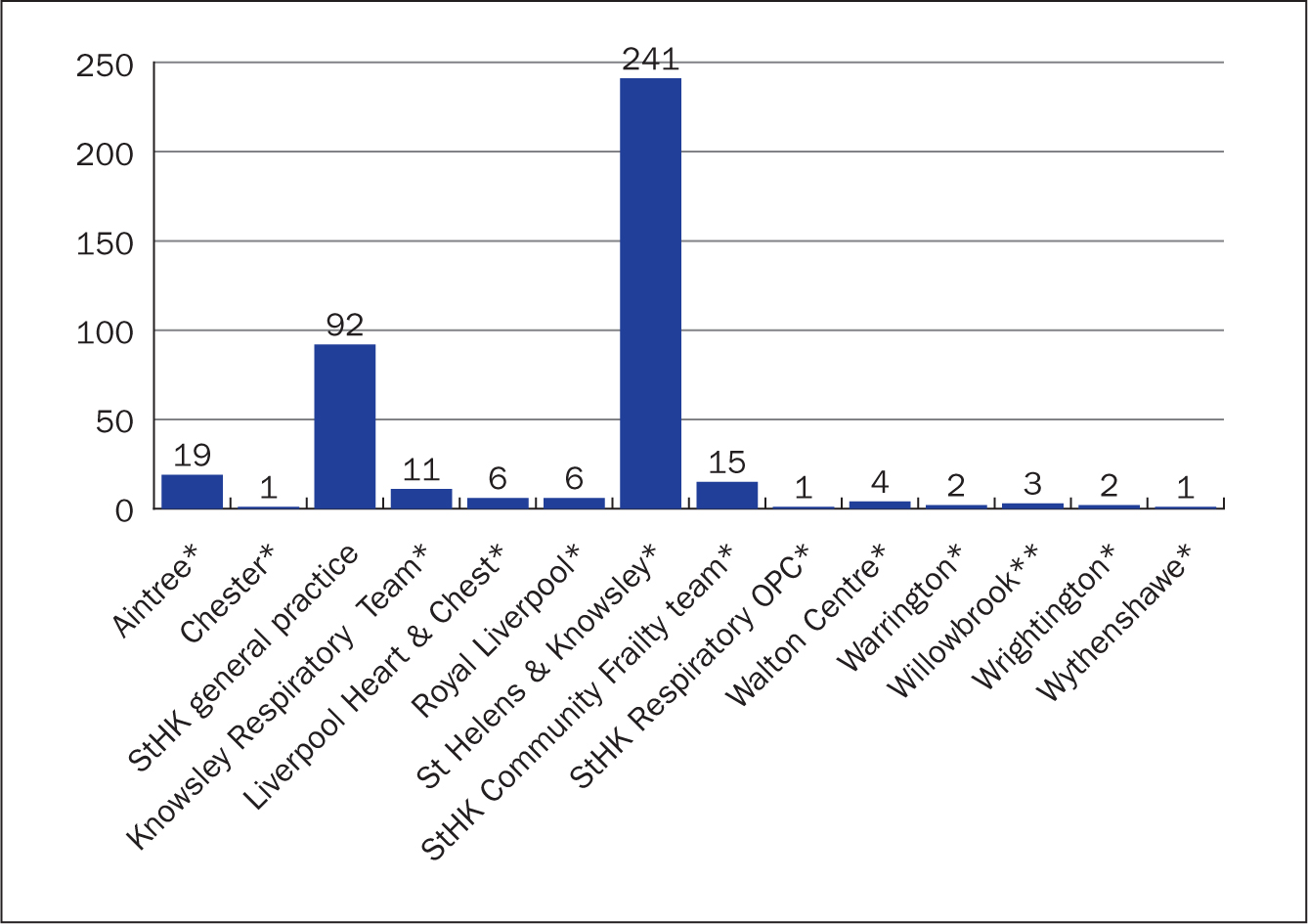 Figure 2. Sources of referrals to the community IV therapy team January 2019 to December 2020
Figure 2. Sources of referrals to the community IV therapy team January 2019 to December 2020 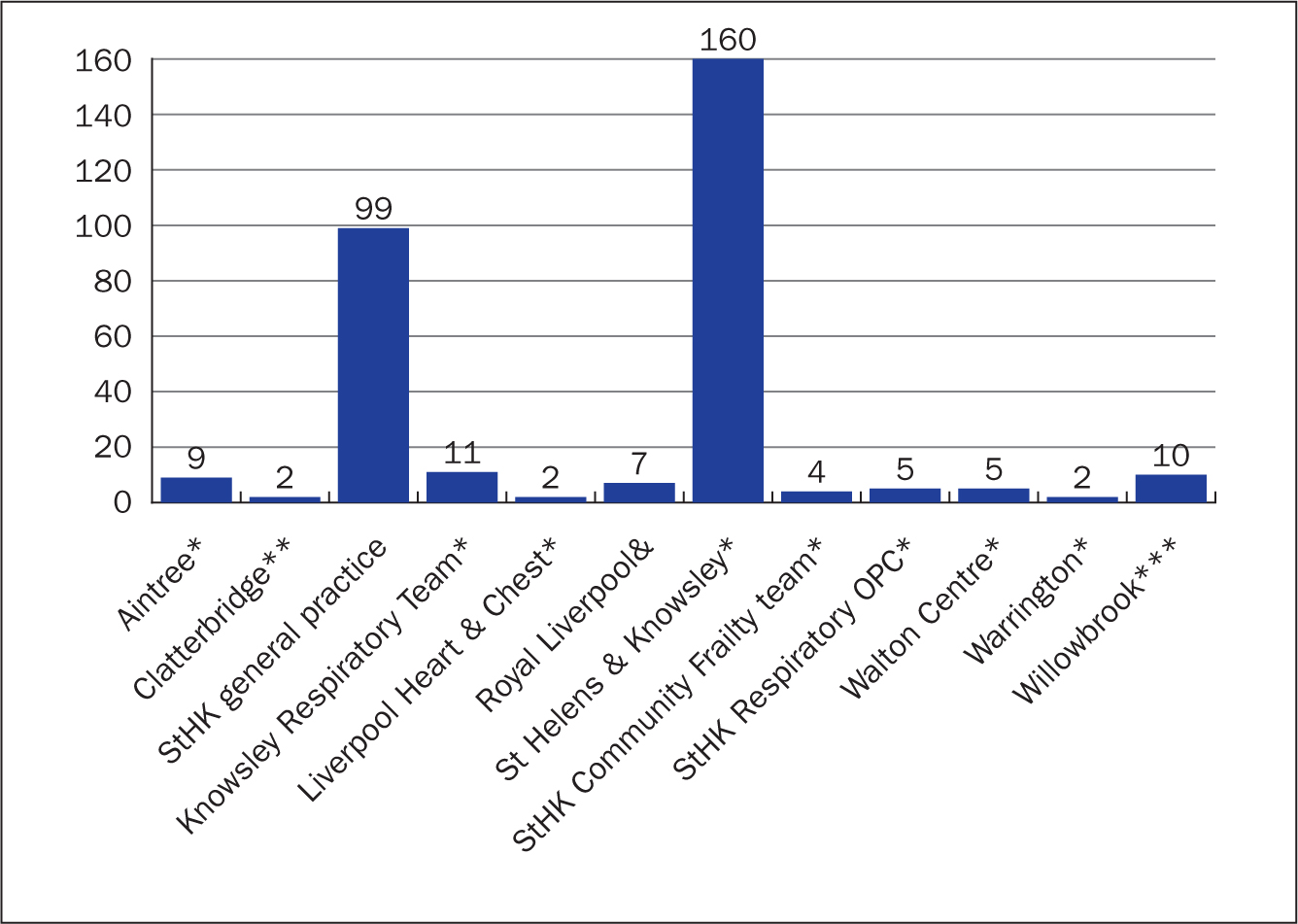 Figure 3. Sources of referrals to the communty IV team during COVID-19 pandemic (March 2020–February 2021)
Figure 3. Sources of referrals to the communty IV team during COVID-19 pandemic (March 2020–February 2021)
This referral pathway for primary care referrals/hospital outpatient clinics allowed patients to receive treatment throughout the early stage of the pandemic without the need for hospital admission, thus freeing up vital capacity within the local acute trust and reducing the potential transmission of the virus by enabling patients to remain in their home environment. While GPs and some specialist nurses have been able to move to predominantly remote consultations, community nursing teams have continued to provide face-to-face care for patients needing support (Bowers, 2020).
Initially this was a community service developed by the primary care trust in 2005. After a local clinical commissioning group (CCG) redesign in recent years, a number of community services have been incorporated into the regional acute trust to form a local care organisation (LCO). LCOs create a global budget through which hospital, community and social care services can be aligned. With the prevention of high-cost emergency admissions heavily dependent on effective health and social care in community settings, there are potentially significant financial rewards associated with creating cost-effective integrated services (Lewis et al, 2010).
COVID-19 first wave
On 20 March 2020 community nursing services in the author's region implemented their emergency business continuity plan. Support was requested from the CIVT, podiatry and continence teams in meeting the demand for patients requiring essential visits in the early part of the COVID-19 pandemic. Treatment room services were non-operational because community clinics were closed in an effort to reduce transmission of the virus. This placed additional demand on the need for face-to-face domiciliary visits. The CIVT team absorbed all pre-existing and new OPAT referrals into the service for a number of months in an effort to provide extra resilience in the community care group.
Inpatient IV access support
Both CNSs within the CIVT team offered inpatient IV access support to the critical care medical emergency team (MET) in anticipation of the team being redeployed to the intensive care unit full time to support the expected surge of COVID-19 patients. Sessions were provided during a 6-week period to ensure the continuation of PICC or midline insertion for hospital inpatients despite the redeployment of the MET. This allowed OPAT referrals to neighbouring teams to continue in a timely manner and freed up vital beds. Inclusion criteria for neighbouring CIVT services required patient to have a midline or PICC before discharge, which may have led to prolonged hospital admission if the inpatient IV access service did not remain operational.
Nurse-led PICC insertion began in the USA in the late 1970s, and this practice was introduced into the UK in the mid-1990s (Dougherty, 2006).
Current UK guidance supports ultrasound-guided insertion of a PICC into the upper arm, which has become an increasingly popular method of placement (National Institute for Health and Care Excellence (NICE) 2002).
Technological changes in recent years have seen ultrasound technology develop into portable and pocket-size ultrasound probes, both wired and wireless, which pair with smartphones and tablets (Rafique and Qadeer, 2021). The ease of portability, sterility, affordability, and integration of innovative technologies included with handheld devices will see their use become commonplace for performing vascular access in the most sterile, quick, efficient and safe manner by practitioners of different specialties and skill levels (Convissar et al, 2021).
Use of a wireless ultrasound scanner during the pandemic enabled the CIVT team to provide midline or PICC insertion in patients in the acute trust in a timely fashion without compromising the capacity of the CIVT service. The portable device was also used for midline insertion for patients with difficult IV access referred from non-hospital-inpatient settings. This invasive procedure was carried out in:
- Community clinics
- GP practices (to reduce the transmission of the virus for patients with no access to transport)
- Nursing homes
- Hospice inpatient wards
- Patients' homes.
Virtual OPAT multidisciplinary team
The acute trust in the author's area of practice has never developed an inpatient OPAT service or funded a dedicated OPAT consultant microbiologist. The clinical and prescribing responsibility for the management of the patient remains with the clinician who makes the diagnosis and assessment of the patient and makes the decision for the patient to commence IV antimicrobials (this could be the hospital or primary care clinician, after discussion with a medical microbiologist) (Pan Mersey Area Prescribing Committee, 2015). Ongoing clinical review and follow-up appointments are arranged on discharge and, if the patient experiences any problems related to the OPAT treatment, the CIVT team liaises directly with the referring team. All non-OPAT-related medical problems are managed by the patient's GP.
Decreased hospital activity levels in the early stages of the pandemic enabled medical microbiologists, antibiotic pharmacists and community IV specialist nurses to meet weekly over a 5-week period to discuss regional OPAT patients. This multidisciplinary team reviewed patient progress and optimised antimicrobial therapy, considering the best agent, dose, route, course, follow up and investigations.
Key benefits have included:
- Safe and cost-effective delivery of the best available therapy with regular monitoring
- Giving patients the best chance of success with the lowest risk of iatrogenic harm (both from OPAT and COVID-19)
- Freeing substantial community IV capacity and providing a forum for issues to be addressed pro-actively
- Antimicrobial stewardship/timely IV-to-oral step down.
Provision of safe, efficacious and cost-effective care in the community is fundamental to the NHS Long Term Plan (NHS England/NHS Improvement, 2019) and must be in accordance with the British Society of Antimicrobial Chemotherapy (BSAC) good practice guidance (Chapman et al, 2019).
A fit-for-purpose OPAT service provides benefits for all key stakeholders. Facilitating the management of patients referred from both primary and secondary care settings, including patients in the community who would otherwise have been admitted to hospital, inpatients discharged from hospital and those who would otherwise attend an outpatient clinic, is intrinsically a complicated and potentially hazardous service. Therefore it requires a multidisciplinary approach to provide governance and safety structures to minimise potential failures in patient management (Chapman et al, 2009).
It is the author's recommendation that robust governance by a specialist integrated OPAT team working across both the acute and community setting is the only way to manage this indispensable service safely, delivering greater efficiency, both for inpatients and outpatients and coping with the ever-increasing demand.
The development of microbiology department-ratified OPAT pathways, for example skin and soft tissue infections for primary care patients, have the potential to further reduce the number of unplanned hospital admissions.
COVID-19 situational analysis
The CIVT team remained fully operational throughout the COVID-19 pandemic. Patients needing once-, twice- and three-times daily medication regimens were all accepted on the service the same day they were optimised for discharge until early December 2020, when increasing demand on community nurses led to some delays in patients being discharged. The use of once- or twice-daily IV medication is common practice in the OPAT setting (O'Hanlon et al, 2017). Antimicrobial selection should be based on appropriate prescribing principles rather than purely dosing convenience (Howden and Grayson, 2002). The recent innovation and availability of portable ambulatory (elastomeric) devices to administer intravenous antibiotics is an attractive option for OPAT services, as these devices enable the patient to receive prolonged infusions and repeated doses of intravenous antibiotics, either at home or in a clinic setting (Allwood et al, 2020).
Elastomerics have been used in the author's area of practice for the past 3 years. Agents used safely after rationalisation by the consultant microbiologist include flucloxacillin, benzylpenecillin, piperacillin with tazobactam, and aztreonam. As well as aminophylline initiated by the regional lung centre specialist on a 6-weekly basis for a patient with severe asthma. Figure 4 shows the various medication regimens administered by the CIVT team during the pandemic.
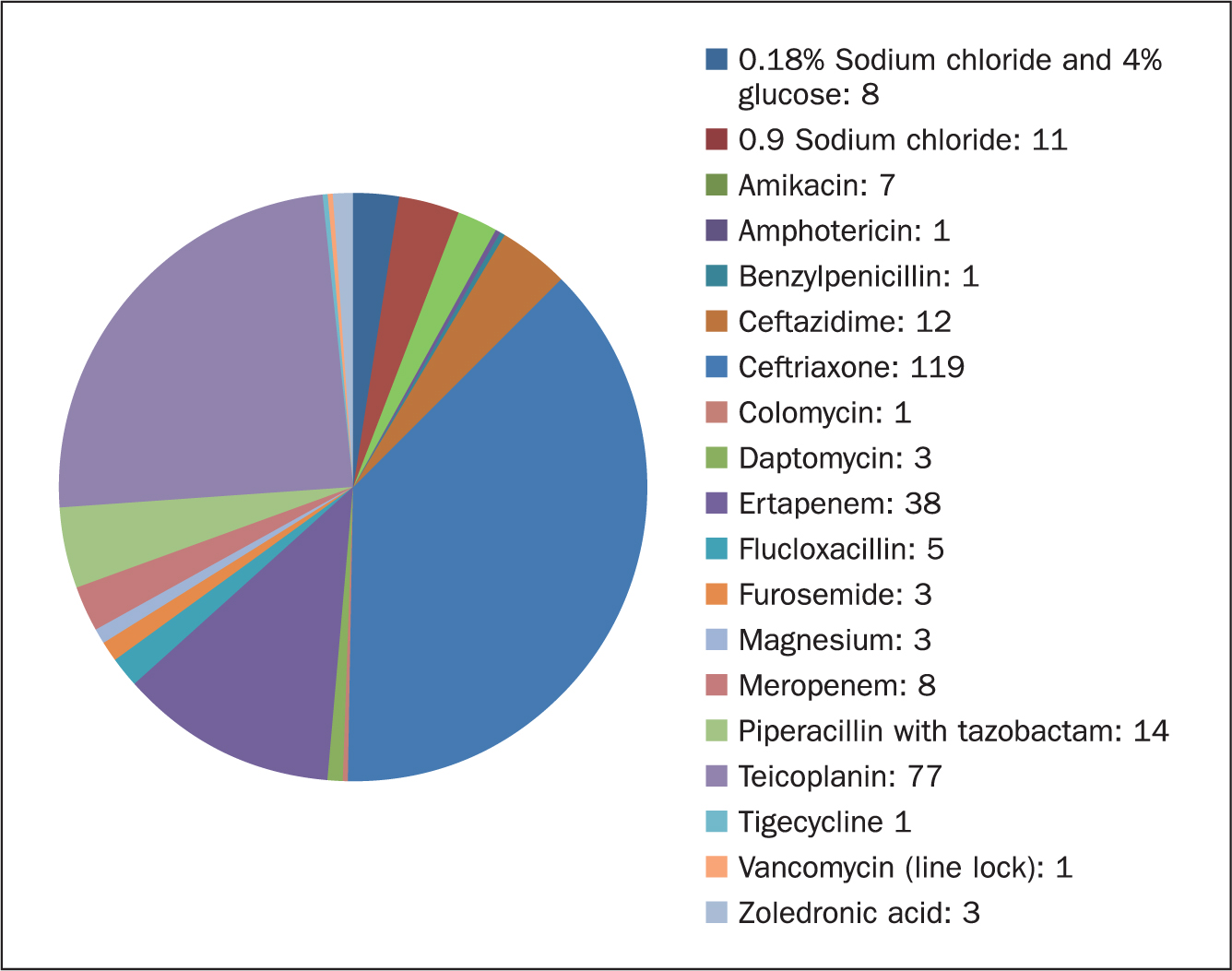 Figure 4. Number of medication regimens provided by the community IV therapy team (March 2020 to February 2021)
Figure 4. Number of medication regimens provided by the community IV therapy team (March 2020 to February 2021)
The CIVT found prefilled infuser devices beneficial during the pandemic because they reduced the amount of time spent inside the patient's home. A combination of minimal preparation time (medication ready diluted), without the need to remain with the patient for the duration of the gravity infusion (usually 30 minutes) helped reduce the face-to-face contact time with patients.
Integrated working
The CIVT team works with the following teams and units:
Ambulatory emergency care: cellulitis
Reschen et al (2020) described ambulatory emergency care (AEC) units providing hospital-level urgent medical services without the need for an overnight stay. This service, termed ‘same-day emergency care’ (SDEC) by NHS England/NHS Improvement, is a key element of the NHS Long Term Plan (2019), aimed at reducing demands on inpatient medical facilities and improving patient experience. The author's local acute trust established an AEC referral pathway for patients with cellulitis in 2012. This is one of the main referral sources for patients referred to the CIVT team.
Same-day response to referrals via AEC prevents unnecessary admission to medical wards and thus frees up vital capacity.
Gastroenterology/nutritional team
Parenteral nutrition (PN) is the delivery of nutrients through the venous system. PN can be administered either in hospital or the patient's home (Alexander et al, 2014). Home parenteral nutrition (HPN) is the primary life-saving therapy for patients with chronic intestinal failure (CIF) (Pironi et al, 2020). Prior to the implementation of the Standard Contract for Intestinal Failure (Adult) (NHS England, 2013) as a national commissioning policy, 12 CIF patients received their HPN nursing care in the author's area under the supervision of the CIVT team and community nurses. In 2017, the consultant physician-led nutritional team at the author's local district general hospital identified a CIF patient suitable for home IV fluid/magnesium replacement outside of the criteria of the HPN framework. The patient was attending the emergency department for parenteral administration of medication every few weeks. The CIVT team invested in an ambulatory pump and accepted the patient on to the caseload for home treatment. Weekly blood samples were obtained by the CIVT team and IV fluid/magnesium replacement administered as prescribed by the nutritional team (NT) after blood results were reviewed. Subsequently individualised clinical management plans for serum urea, electrolyte and magnesium levels have been set by the NT team so that the CIVT team are aware of what weekly IV therapy to administer. This model of care has led to the patient having only one admission to the acute trust (to date) with electrolyte imbalance. Another six lifelong CIF patients have also been accommodated in the service, using the same treatment regimen, with ongoing support provided by the NT.
Community frailty team
The NHS Five Year Forward View requires local and flexible community care (NHS England, 2014). The British Geriatrics Society (2018) recommends that people with frailty should be managed by responsive community services. In the author's region this has led to the development of a consultant geriatrician-led multidisciplinary frailty community service that is integrated with the inpatient frailty unit. Service delivery includes consultant geriatrician domiciliary assessment and provision of non-acute inpatient care for the cohort of people who attend the trust, but do not have ongoing acute medical needs but need multidisciplinary team reablement and discharge planning support. IV treatments initiated by the frailty team without the need for admission into the hospital include fluids, diuretics and antibiotics.
Community palliative care team
Hypercalcaemia is the leading malignancy-related metabolic complication in hospital and is recognised as a medical emergency due to the risk of hypovolaemia, dehydration, coma and cardiac arrest. Adequate hydration with IV saline is crucial in the initial management and effective treatment also requires pharmacological IV agents to treat the underlying cause of increased calcium release from bone (Berger et al, 2013). During the pandemic the CIVT received an increase in the number of referrals from the community palliative care team compared to previous years. Patients wishing to receive treatment at home as their preferred place of care, received therapy at home for hypercalcaemia, dehydration and infection with the support of the CIVT team and community nurses throughout the pandemic.
Community respiratory team/respiratory outpatient clinic
The British Society Thoracic bronchiectasis guidelines recommend IV antibiotics are considered when patients are particularly unwell, have resistant organisms or have failed to respond to oral therapy (Hill et al, 2019). Moreover, although there is extensive experience of OPAT with antibacterial agents, there is a dearth of evidence regarding the use of parenteral antifungal agents in OPAT (Rae et al, 2019). In the author's area of practice the hospital-based respiratory physicians have been key stakeholders in the development of the OPAT service since 2005. Initially, patients accessed the service through early supported discharge; however, referrals direct from the respiratory outpatient clinic have reduced the need for planned inpatient admission in recent years. Patients are accepted on antimicrobial regimens up to three times daily and patients have received antifungal treatment safely in their home environment in recent years. Amphotericin B (prescribed for aspergillosis) was administered to a patient at home in the early stages of the pandemic to facilitate their discharge from a respiratory ward. In addition, two other patients were treated at home with micafungin for aspergillosis infection.
Out-of-hospital integrated working helped reduce the incidence of clinically vulnerable patients attending the hospital during peak COVID-19 times.
Areas for development
Figure 5 shows all patient contacts carried out by the CIVT team before and during the pandemic and Table 1 shows bed days and costs saved by referral patients to the community IV team.
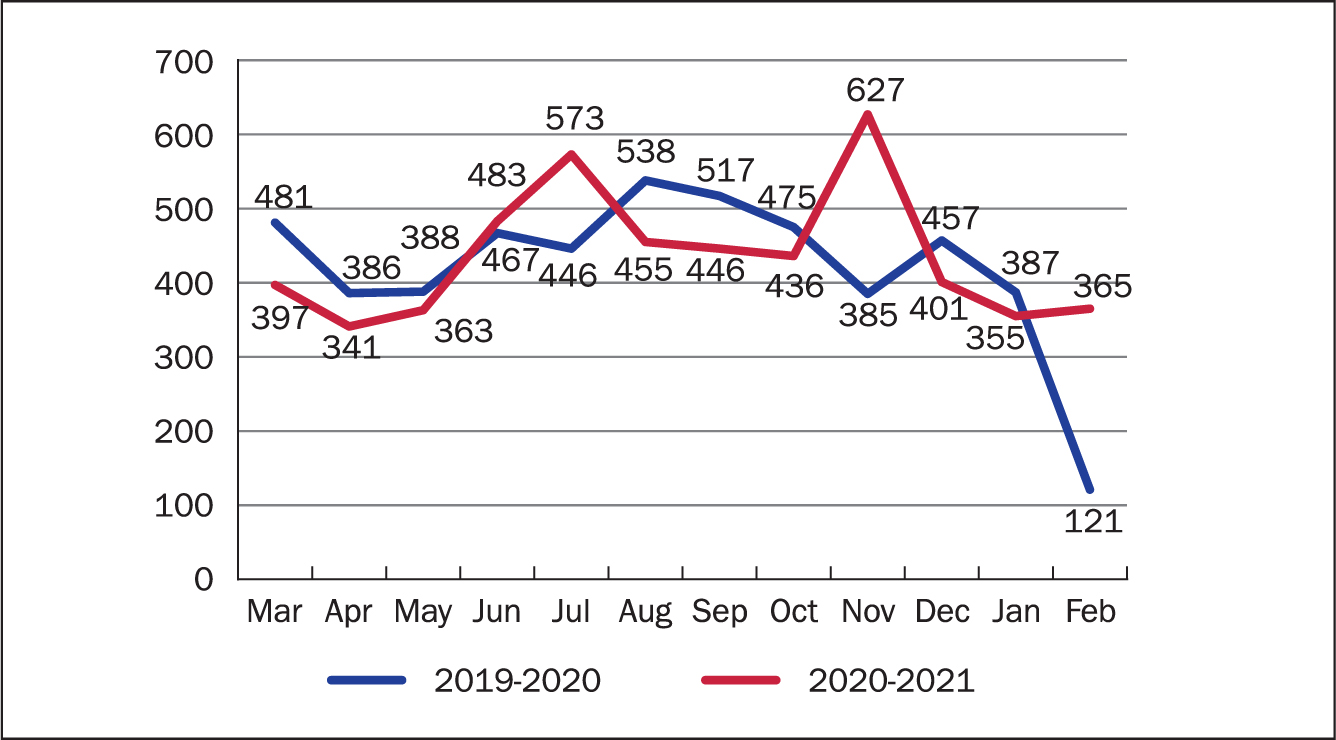 Figure 5. All patient contacts carried out by the Community IV Therapy Team before and during the COVID-19 pandemic
Figure 5. All patient contacts carried out by the Community IV Therapy Team before and during the COVID-19 pandemic
Table 1. Bed days saved by referral to community IV team
| Year | Patients referred | Bed days saved | £ saved |
|---|---|---|---|
| 2010 | 116 | 2095 | 628 500 |
| 2011 | 181 | 2831 | 849 300 |
| 2012 | 223 | 3706 | 1 111 800 |
| 2013 | 333 | 5285 | 1 585 500 |
| 2014 | 343 | 7290 | 2 187 000 |
| 2015 | 631 | 8141 | 2 442 300 |
| 2016 | 696 | 9625 | 2 887 500 |
| 2017 | 486 | 8036 | 2 410 800 |
| 2018 | 438 | 6975 | 2 092 500 |
| 2019 | 432 | 5829 | 1 748 700 |
| 2020 | 343 | 4542 | 1 362 600 |
| Total | 4222 | 64355 | 19 306 500 |
The administration of IV diuretics in a community setting is clinically safe, cost-effective, and valued by patients and carers, with the right infrastructure and resources, existing heart failure teams can provide a service that enables patients to have IV diuretics delivered safely and effectively in the comfort of their own homes (Blue, 2015). Within the author's region in 2019 the consultant cardiology-led community heart failure team, CIVT team and local CCG had developed a community IV diuretic pathway that was due to be launched as a 6-month pilot during 2020. Unfortunately, this project has been paused due to the pandemic, but will hopefully be revisited in early 2022.
Ferric carboxymaltose (Ferinject) is a new novel non-dextran-containing complex of intravenous iron that may be of significant benefit for use in the outpatient department or in a community setting as a result of its rapid and high-dose replacement of depleted iron stores in patients with chronic kidney disease (CKD), as well as in various other adult populations with iron deficiency anaemia (Lyseng-Williamson and Keating, 2009). CKD has an estimated prevalence in England of 15% in people aged 35 years and over (Gaskell et al, 2008). In the author's region, IV iron was administered safely to patients at home until the 2014 Medicine and Healthcare products Regulatory Agency (MHRA) strengthened recommendations regarding hypersensitive reactions (MHRA, 2014). The emerging view is that serious adverse events have declined with newer IV iron preparations (Qunibi, 2010), which may lead to the provision of iron replacement by GPs in the near future.
Home blood transfusion schemes help oncology patients avoid unnecessary emergency admissions and improve the capacity of hospital day units (Benson, 2006). Despite this service being provided successfully by a neighbouring trust, this area of practice has not been developed in the author's area of practice.
The advent of ambulatory infuser devices (using elastomeric pumps) now enables patients to receive prolonged infusions of chemotherapy at home; patients are usually connected to these devices at the cancer centre and then visited by community nurses at the end of infusion for disconnection (Nabhani-Gebara and Salman, 2019). Future models of care could see NHS staff attend the patient's home to start this treatment rather than attend an oncology centre at an acute trust.
Conclusion
IV therapy skills and expertise developed by established community OPAT services can be used in the development of other areas of infusion therapy in providing out-of-hospital care. The discharge model promoted by the DHSC (2020) during COVID-19 changed the way that many services operated on a short term basis in an effort to free up hospital capacity. With the right investment, clinical support and relevant pathway development from CCGs and LCOs, care closer to home can be the new standard for patients across the UK.
IT systems and new technology (video calls, consultations and conferencing) enabled patients, healthcare providers and commissioners to work collaboratively throughout the global pandemic. These new ways of working need to continue and services proactively develop to ensure that traditional communication barriers between acute and primary care in the NHS can be overcome to provide truly integrated care. The ‘new normal’ for post-pandemic NHS community services should pose the question: ‘why not commence treatment at home, why not today and without the need for hospital admission?’
KEY POINTS
- Integrated working enabled a community IV therapy team to extend its service provision to other IV therapies in addition to antimicrobials
- Treatment can be initiated in the community without the need for hospital admission
- Use of new digital technologies can improve communication between acute and primary care teams
- Portable ultrasound scanners aid in the management of patients with difficult IV access in primary care
CPD reflective questions
- What integrated services are already established in your local area—how well are they working and how could they be improved?
- How can integrated working improve the patient journey and experience?
- When would hospital admission rather than community care be appropriate?