

Encephalitis is inflammation of the brain tissue (Solomon et al, 2007), the causes of which in Western Europe include viruses, such as the herpes simplex virus (HSV), bacteria, such as Toxoplasma gondii, and auto-immune causes, such as voltage gated potassium channel-complex antibody-associated limbic encephalitis (Granerod et al, 2010). In England, encephalitis has an annual incidence of 5-8 cases per 100 000 of the population (Granerod et al, 2013) and in a significant proportion of patients, no cause is identified (Granerod et al, 2010). Encephalitis inflames the brain tissue, leading to brain injury. In some cases it leads to death, as such encephalitis is a neurological emergency. Encephalitis can affect any age group, and the signs and symptoms include fever, headache, sensitivity to light, memory loss and acute confusion. All causes of encephalitis can leave people with significant disability, however, prompt treatment with aciclovir significantly reduces mortality and morbidity (Sköldenberg et al, 1984; Whitley et al, 1984; Richie and Josephson, 2015; Ellul and Solomon, 2018; Frackowiak et al, 2019; Ellul et al, 2020).
As a result of the brain damage that encephalitis can cause, encephalitis can result in a high economic and social burden to both patients and society (Solomon et al, 2012; Easton, 2016): patients may not only be unable to work at all or to the same level as previously, but they may also need long-term care and support with activities of daily living. This can negatively impact their families' economic status, and patients post-encephalitis may also rely directly on family members for day-to-day help and support.
In their follow-up prospective study, Hokkanen and Launes (1997) found that six out of 11 adults affected by encephalitis had long-term psychiatric and cognitive impairments. Easton et al (2007) found that, although 96% of patients with encephalitis had ongoing complications, 33% were discharged without any planned follow-up. There is a lack of guidance both on where patients with encephalitis should be nursed and on how to provide appropriate nursing care. These important points provided the focus for this study.
Mainstream provision of services can struggle to accommodate the complexity of these patients' care, however, Easton et al (2007) stated that less than 40% of these patients are cared for on specialist neurological wards, which means that many are cared for in non-specialist settings. Solomon et al (2012) pointed out that not only are there no guidelines on the nursing care of such patients, but there is no clear evidence of in which settings nursing care should be provided. Patients currently tend to be cared for in general medical wards, specialist neurology wards/neurology centres, infectious diseases (ID) wards and intensive care. Easton (2018) highlighted the role of primary care in diagnosing encephalitis and managing the physical sequelae post encephalitis.
Literature review
A literature search was carried out to identify if there were any original research papers of the nursing care of patients with encephalitis. The databases Medline, Cinahl, Embase, British Nursing Index and Scopus were searched. The search strategy included the terms ‘encephalitis’, ‘nursing’, ‘care’ and ‘challenges’. No date range was set on the search, because it was already known from previous searches in this area that the number of studies was likely to be minimal. The inclusion criteria applied as part of the search were that articles had to be written in English, be original research published in a peer-reviewed journal, and for the purposes of this study they had to concern adults, rather than children. Exclusion criteria were studies on non-acute encephalitis, systematic reviews and literature reviews. No original research papers on the nursing care of patients with encephalitis were found.
Because of this, a second literature review was carried out to set this research in the broader context of caring for patients with other neurological conditions who develop confusion, as this is often the case for patients with encephalitis. The search strategy included the terms ‘neurological conditions, ‘delirium’, ‘confusion’, ‘nursing’ and ‘care’. The inclusion criteria for the second search were that articles had to be written in English, have been published in a peer-reviewed journal, and had to concern adults rather than children. This revealed a broad body of evidence of how confusion is commonly encountered in patients with neurological conditions, how the care of these patients can be challenging and how it can often be hampered by staff shortages. Studies in this field highlighted the importance of nurses in managing confusion to maintain the safety of neurology patients with confusion, and to treat it (Bélanger et al, 2011; Baker et al, 2015; Kristianson et al, 2019; Zipser et al, 2019; Wilson et al, 2020). Certain articles identified in the search also showed how nurses caring for these patients often felt that their ability to prove adequate care can be hampered by staff shortages or understaffing (Bélanger et al, 2011; Baker, et al 2015; Kristianson et al, 2019).
Methodology
Aim
The primary aim was to explore the experiences and perceptions of registered nurses providing care to adult patients with encephalitis, from admission to hospital through to discharge.
Design
This study was a qualitative exploration that used semi-structured interviews. The theoretical framework guiding the study was a qualitative, phenomenological approach. The key concepts considered for the basis of this research are the traditions of phenomenology, a philosophy and method that focuses on understanding the lived experience (Gadamer, 1989; Heidegger, 1998; Vandermouse and Fleming, 2011; Englander, 2012). Despite descriptions of a phenomenological movement, it is generally accepted that there are broadly speaking two traditions of phenomenology (interpretive and descriptive), although Crotty (1996) pointed out that there is diversity within these traditions.
This study followed the tradition of interpretive phenomenology, as it was accepted that the role of the researcher as a research nurse in brain infections at the recruiting hospital site, was likely to have an impact on the research process and interpretation of the findings.
Participants
A sample of eight registered nurses were recruited from one secondary hospital using purposeful sampling. This was a large, city centre university teaching hospital, with a large emergency department (ED), theatres, an intensive care unit (ICU), and surgical and medical wards. The hospital also had two infectious diseases (ID) wards. It did not have any dedicated neurology wards or units. The lead researcher (CG) approached potential participants to invite them to take part. They were given verbal and written information about the study and had at least 24 hours to decide if they wanted to participate. Before the interviews took place participants gave written consent.
The inclusion criteria were:
- The participant was a registered general nurse (RGN), employed by the hospital trust being used for the study
- Experience of having nursed at least one patient with encephalitis.
Participants were recruited by identifying wards commonly involved in the acute management of encephalitis, gained through the researcher's role as a research nurse in a multicentre prospective study looking at the outcomes of encephalitis across the UK.
Apart from one nurse who was based on a medical assessment unit (MAU), the nurses in the study had all nursed patients with encephalitis relatively regularly, at least three to five times a year. The hospital was not a specialist neurological facility, but it received specialist referrals for these patients due to its ID unit. Patients with encephalitis are ideally nursed on the hospital's ID unit, unless they require critical care or there are no beds on the ID unit. The nurses all had at least 5 years' experience, with the most senior nurse interviewed having over 20 years' experience.
Participants ranged from staff nurses to ward managers, and all but one worked on ID wards, with the remaining participant working on an MAU. Table 1 shows participants' demographic details. The authors aimed to recruit 10 participants, but due to time constraints only eight participants were recruited.
Table 1. Patient demographics
| Subject ID | Sex | Nurse grade | Area worked |
|---|---|---|---|
| 001 | Female | 5 | Infectious diseases |
| 002 | Female | 5 | Infectious diseases |
| 003 | Female | 7 | Infectious diseases |
| 004 | Female | 5 | Infectious diseases |
| 005 | Female | 5 | Infectious diseases |
| 006 | Female | 5 | Infectious diseases |
| 007 | Female | 5 | Infectious diseases |
| 008 | Female | 5 | Medical assessment unit |
Data collection
Data were collected using in-depth, semi-structured interviews, between October 2014 and August 2015. Semi-structured interviews were used because they are the most appropriate collection method for the type of data the study aimed to produce. This methodology ensured that data on all the study objectives were covered, as well as allowing responses to be fully explored and the researcher to respond to relevant issues that were raised spontaneously by a participant (Ritchie and Lewis, 2009).
Interviews took place at the hospital site, in a quiet room, away from the work environment, and lasted for about 60 minutes. This gave enough time for in-depth discussion and for an exploration of key issues. Interviews were recorded verbatim using an audio-recorder.
Ethical approval
Ethical approval was gained from the university that was the study sponsor, and local approval gained from the hospital site where participants were recruited. Because the study was interviewing staff members only, NHS Research Ethics Committee approval was not required.
Data analysis
The method of data analysis used for this study was framework analysis. One of the reasons for selecting this method was because it provides a clear audit trail (Flick, 1998).
Interviews were transcribed in full by the researcher (CG). This meant that the researcher was very familiar with the data before analyses began. Stage 1 analysis involved immersion by reading and re-reading the transcripts. Stage 2 involved developing a theoretical framework by identifying recurrent and important themes. The recurring themes identified in stage 2 were added to a chart on paper as part of the analysis. Stage 3 consisted of indexing and pilot charting.
The draft framework developed in stage 2 was applied back to the transcripts, and a refined framework devised. In stage 4 the data were summarised in an analytical framework. The material was reduced to understandable but brief summaries of what had been said by each participant. In stage 5, the final conceptual framework for the analysis was assembled, which included the merging of some of the overlapping sub-themes. Figure 1 provides a diagram of the analytical framework. Table 2 summarises each stage of the analysis.
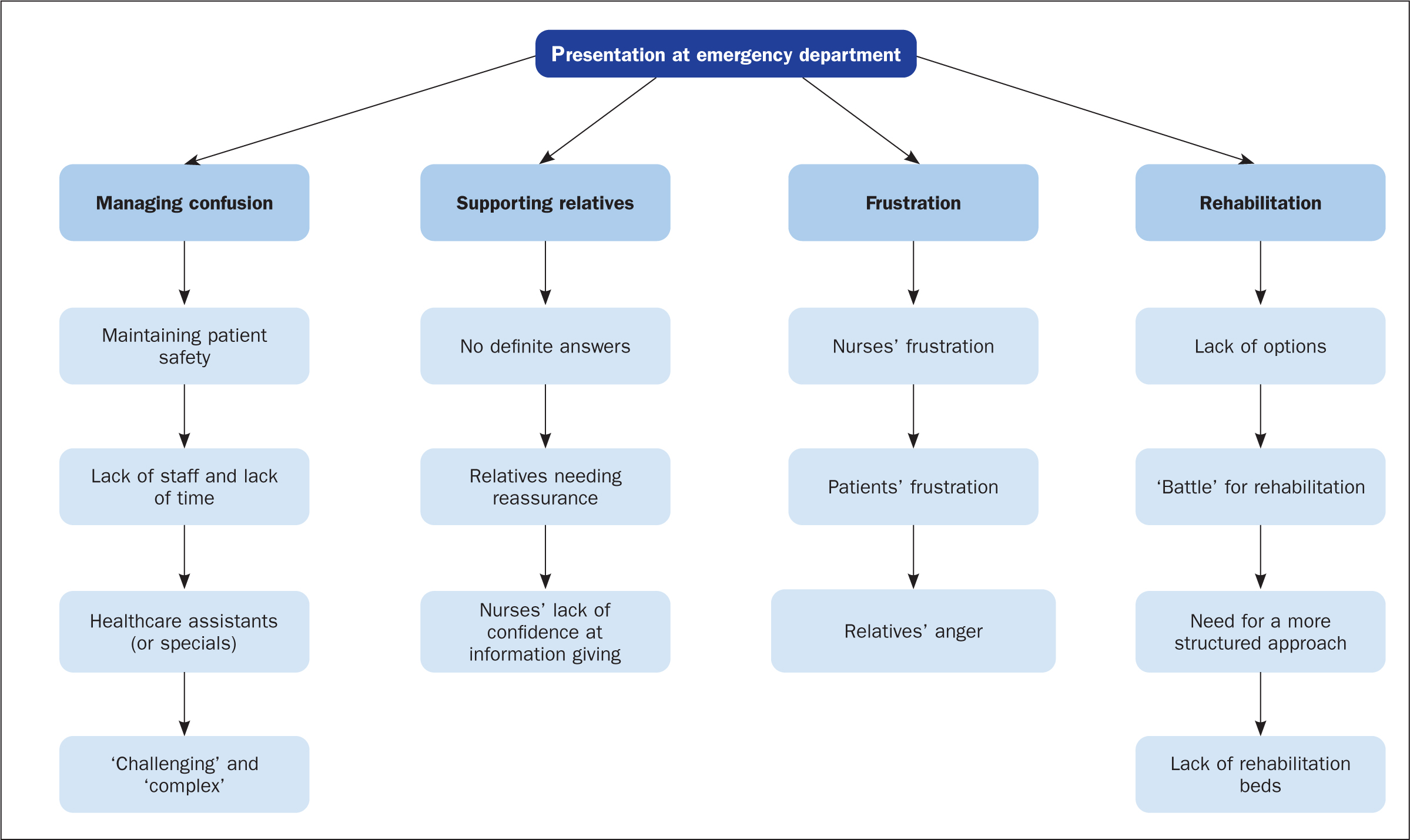
Table 2. Stages of analysis
| Stage | Activity |
|---|---|
| Stage 1 | Detailed reading of transcripts |
| Stage 2 | Theoretical framework developed |
| Stage 3 | Indexing of transcript data |
| Stage 4 | Summary of data |
| Stage 5 | Final conceptual framework and merging of sub-themes |
Validity and reliability of the analysis
The validity and reliability of the findings was ensured by having two independent researchers (separate from the authors) experienced in working with phenomenology independently code a sample of the data. These independent analyses produced similar themes. The rest of the coding undertaken by the lead researcher was also reviewed by the second researcher (CG and AE) for validity and reliability. The two researchers discussed and reached an agreement when interpretation of the themes differed. The audit trail produced by framework analysis also gave rigour to the work, because it gave a clear written record of the steps taken in the analysis, and the findings and decisions made at each of the five stages.
Results
Key findings
The data collected showed that nurses:
- Lacked knowledge of encephalitis to enable them to care for these patients confidently
- Lacked time to give patients the level of care that they required
- Experienced a lack of access to specialist neuro-rehabilitation for these patients.
These findings are consistent with findings in the wider literature on the management of acute confusion and nursing shortages generally.
The three key findings, each of which is discussed in more detail below, were derived from the following four primary themes that emerged during the data analysis (Figure 1):
- Managing confusion (for example, the nursing challenges this poses)
- Supporting relatives (for example, explaining the potential for life-long brain damage in their relative)
- Frustration (for example, nurses' frustration with staff shortages making it difficult to give these patients the level of care required)
- Obtaining appropriate rehabilitation for the patients (for example, lack of beds in neuro-rehabilitation centres)
Lack of knowledge
It was clear from the interviews that all the participants felt that they lacked knowledge of encephalitis, which hampered their confidence in care and information giving. It was generally recognised that, although an uncommon condition, a diagnosis of encephalitis required rapid diagnosis and nurses did not always recognise the nursing needs required to care for a patient with encephalitis were not always recognised. This is an important finding because, if nurses are not aware of patient's needs, it could mean that they get suboptimum care.
For example, one participant, describing how much more difficult it was to plan appropriate care for patients with encephalitis when they become acutely confused, stated:
‘It's trying to work out what their needs are … it's quite challenging … it's hard knowing exactly what their needs are …’
Subject 001
When describing her biggest fear in caring for patients with encephalitis, another nurse described how scared she felt about her lack of knowledge about the condition, and how this hampered her communication with relatives:
‘… lack of knowledge [is my biggest fear]. I think that scares me. When I don't know something I don't like it, I get scared of it. I don't like not being able to … if a relative asks me what's wrong and I can't answer it or in ward round one of the doctors goes [what sounds to me like] blah blah blah and I'm saying what [does your diagnosis mean]?’
Subject 003
Lack of time
The finding regarding lack of time emerged from the four themes—managing confusion, supporting relatives and trying to arrange rehabilitation—all require significant time, which the nurses in this study felt they lacked. All study participants highlighted how much time was needed to care for patients with encephalitis and how short of time they were as nurses. They also said that this was often compounded by staff shortages, which is an important finding: it shows how many patients with encephalitis may be suffering because of staff shortages, and the lack of consideration given when allocating nurse caseloads to how much time is required to care for patients with encephalitis.
For example, one participant noted the dependence of acutely confused patients with encephalitis on nurses for nearly all their activities of daily living, such as feeding, hygiene and dressing:
‘In general, these patients take up a lot of time, anyway as they require a lot of care. But, quite often, when they're confused, they require full care and everything.’
Subject 005
Another participant expressed concern over the lack of staff and one-to-one healthcare assistants (HCAs) (or specials) for patients that need such individualised care. This appeared to have a strong impact on her perceived ability to provide good-quality care to patients with encephalitis on her ward.
‘… our ward is one of the ones [where] we do need staff, so when we get, you know, encephalitis patients it's frustrating. We don't get the staff we need.’
Subject 003
Lack of access to rehabilitation
The need for patients with encephalitis to have access to high-quality and appropriate rehabilitation was strongly identified by all respondents. Paradoxically, each of the participants also felt strongly that patients rarely received the rehabilitation that they needed. This is an important finding because it shows that the lack of access to appropriate services for patients affected by encephalitis was a common theme, and this could mean that the recovery of many of these patients' recoveries is limited due to lack of rehabilitation services.
Subject 005 described the general difficulty of getting patients into rehabilitation facilities by saying that ‘[to get rehab] … it's just too hard.’
Subject 007 echoed the views of previous participants when she described the lack of bed availability in rehabilitation facilities. This was a recurring discussion point throughout the interview.
‘Yeah, it's difficult. There's only so many beds for so many people. Some people can go and do outpatient clinics. They can go to centres, like, every day. They can do some stimulation and do stuff with them that they need. But long-term, yeah, it can take a fair while.’
Subject 007
Discussion
It is recognised that the study was exploratory in its findings. It did, however, produce some tentative new knowledge on the challenges faced by nurses when caring for patients with neurological conditions such as encephalitis. It has achieved this by identifying four overarching themes:
- Managing confusion
- Supporting relatives
- Frustration
- Rehabilitation.
However, it could be considered that by helping their patients to become more independent in their activities of daily living, nurses themselves are playing a part in that rehabilitation, but perhaps the nurses in this study did not recognise this. These four themes led to the three key findings regarding the lack of time, knowledge and rehabilitation.
Although the study focused on encephalitis, it is interesting that the findings reveal problems that are common with other conditions, such as acute confusion more generally and other traumatic or acquired brain injuries. Problems with lack of staff and lack of time to give optimum nursing care are well documented in the literature for many neurological conditions, as is the need for increased knowledge for nurses in caring for these patients, and better access to rehabilitation for patients. The challenges that nurses face when providing care for patients with the condition have much in common with those encountered with regard to other neurological conditions.
There is a misconception that encephalitis is a relatively rare condition, but in reality it has a higher incidence than neurological conditions such as multiple sclerosis and bacterial meningitis (Easton et al, 2007). This is an additional reason why awareness and training about encephalitis, especially for nurses, is ever more important, as the findings of this study suggest. Although nurses are likely to have had some training on multiple sclerosis, bacterial meningitis and acute confusion, they are most unlikely to have received education about encephalitis and training in the care of affected patients, unless they work in a specialist neurology unit.
This consequently poses the question of whether the findings of this study need to be examined within the much broader picture of other neurological conditions, an area where nursing care is also challenged by staffing issues, the need for more training and knowledge provision for nurses, and the lack of access to rehabilitation due the shortage of facilities. The findings of this study are in keeping with other evidence that has been reported in the context of patient confusion in other neurological conditions (Bélanger et al, 2011; Baker et al, 2015; Kristianson et al, 2019; Wilson et al, 2020).
It could be argued, therefore, that this work has provided some evidence towards developing a new theory on the nursing care of patients with encephalitis. However, it could also be argued that the findings of this study must be considered within a much bigger picture along with other neurological conditions, and perhaps any future work in this area could assess these findings within such a wider context.
The findings within the broader context of confusion and neurological conditions
It is necessary to relate the findings of this study to the existing evidence on confusion and neurological conditions. The findings of the study are in accordance with findings reported in the existing literature on the need to both screen for, and manage, delirium effectively (Bélanger et al, 2011; Baker et al, 2015; Kristianson et al, 2019; Zipser et al, 2019; Wilson et al, 2020). For example, Lamond et al (2018) highlighted the importance of screening for delirium consistently in the intensive care setting. Yevchak et al's (2012) study has particular relevance to the findings of this study because they ran a pilot focus group with nurses working in acute care settings, concluding that more needs to be done to promote evidence-based and non-pharmacological approaches to caring for patients with delirium.
The findings of the present study also have relevance to the literature on nursing shortages more generally. Buchan and Aichen (2008) argued that nursing shortages have an impact on clinical practice and health service delivery, and Oulton (2006) highlighted that nursing shortages are a global problem. The findings of this study therefore have important relevance to the current literature on managing acute confusion and nursing shortages in all clinical fields.
Limitations
The main limitation of this study was its small sample size. This makes it impossible to generalise its findings to the broader nurse population. However, the aims were to identify key themes and topics that are transferable and applicable to the participants under study, which was achieved. Another limitation is that, due to the need to recruit participants who could provide in-depth data, purposive sampling cannot guarantee how representative the subjects were. There is also a lack of heterogeneity within the sample in terms of gender, seniority and clinical areas of work.
Conclusion
In conclusion, this study has provided an exploratory start to look at the challenges of providing high-quality nursing care to patients with encephalitis. The nurses interviewed for the study lacked time, knowledge and access to rehabilitation when caring for patients with acute encephalitis. The findings of the study agree with current literature on managing acute confusion and nursing shortages generally. The implications for practice from this study are that it underlines the need for adequate staffing, training and better access to rehabilitation for patients with neurological conditions such as encephalitis.
Although neurological rehabilitation is generally in short supply, it is often the case that specialist neurology centres have better access to this than tertiary hospitals. Future research into the challenges of nursing patients with encephalitis should perhaps consider the wider context of neurological conditions, to produce findings that are more widely generalisable.
KEY POINTS
- This work adds to the knowledge on the nursing care of patients affected by encephalitis by highlighting how difficult they find managing care, if patients become acutely confused
- The findings show that nurses feel they lack the knowledge and time to give adequate support to patients with encephalitis and their relatives
- Nurses in this study reported difficulties accessing appropriate rehabilitation
- The findings are in keeping with current literature on the difficulties for nurses when managing acute confusion, particularly when this is compounded by nursing shortages
CPD reflective questions
- Are there any challenges that are common to the care of patients with acute confusion?
- As nurses, how could we work with charitable sectors to help to support the relatives of patients with brain infections?
- How have you coped with having to explain to patients and relatives when there is a potential for long-term brain damage?