

Myeloma is an aggressive B-cell malignancy resulting from the uncontrolled production of plasma cells in the bone marrow. Normal plasma cells help to fight infection by making antibodies that help recognise and attack germs. Malignant plasma cells accumulate in the bone marrow, causing low blood counts and can also cause direct or indirect damage to other organs such as the kidneys and bones, which can lead to kidney failure, pathological fractures and high levels of calcium in the blood. In the UK, there are around 6000 new cases of myeloma diagnosed annually (Cancer Research UK, 2023). In Europe, the estimated number of new cases of myeloma in 2020 was 6.8 per 100 000 (Dyba et al, 2021).
A multitude of drugs used alone or in combination are now approved for use to treat this complex disease and nurses require knowledge and skills in recognising and managing new side effects associated with these treatments. This article presents an overview of some of the newer and recently approved drugs and the important side effects that have been associated with them.
Diagnosis
When suspicion of myeloma is raised, a number of investigations are required to confirm the diagnosis. These include bone marrow aspirate and biopsy. The presence of plasma cells greater than 10% leads to a diagnosis of myeloma, in addition to the evidence of end-organ damage namely hypercalcaemia, renal impairment, anaemia or lytic bone disease (known as CRAB symptoms) (Rajkumar, 2020). Additionally, other indicators include the presence of one or more biomarkers (a myeloma defining event (MDE)) such as >60% plasma cells in the bone marrow, an abnormal serum free light chain ratio (SFLCR) (0.01) and more than one focal bone lesion on the imaging using whole body MRI.
A whole-body low-dose CT scan will reveal any destruction/damage in the form of lytic lesions. A 24-hour urine collection will identify and quantify the level of light chains (Bence Jones protein) being excreted. A number of blood tests determine the diagnosis and facilitate the staging and prognosis, such as full blood count (FBC), an oncology profile, which includes kidney, liver and calcium levels as well as infection marker (C-reactive protein (CRP) levels and lactate dehydrogenase (LDH)), serum protein electrophoresis (SPEP), SFLCR, and beta-2 microglobulin.
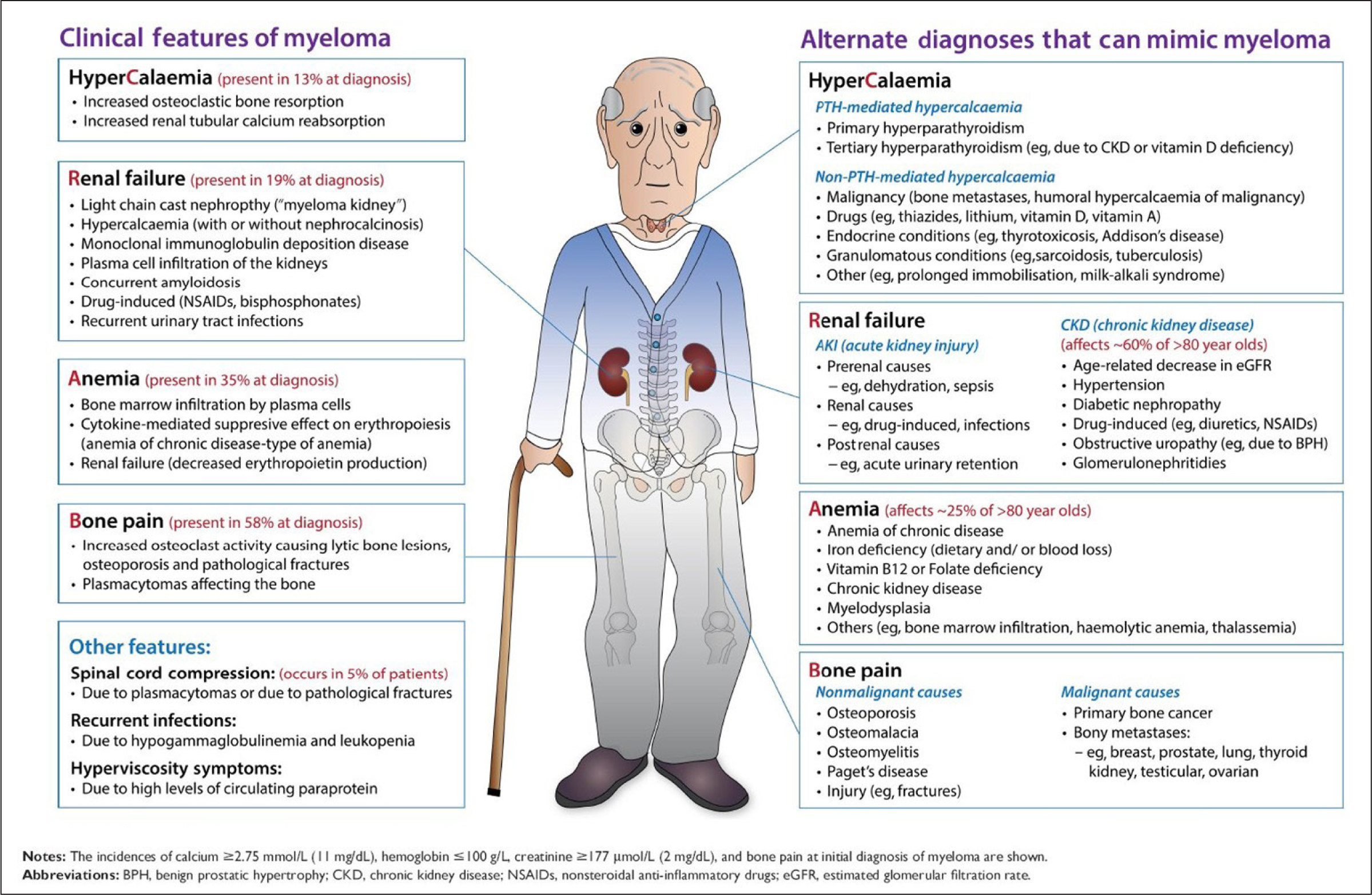
The clinical presentation of myeloma can vary from person to person and can mimic other conditions (Figure 1). It can be diagnosed by chance on a routine medical check-up or while undergoing tests for other procedures/investigations. Most patients with symptoms of myeloma present will have bone pain, fatigue due to anaemia, recurrent infections or renal impairment and hypercalcaemia (Bird and Boyd, 2019).
Staging and prognosis
Staging and prognosis are evaluated using the Revised Multiple Myeloma International Staging System (R-ISS), which divides patients into three stages (Palumbo et al, 2015). R-ISS combines the original ISS with genetic markers and lactate dehydrogenase and can prognosticate newly diagnosed multiple myeloma. The tool can be accessed online (https://www.mdcalc.com/calc/3842/revised-multiple-myeloma-international-staging-system-r-iss). The knowledge of cytogenetics has impacted the staging and prognosis of the disease. Cytogenetics examines the mutations of the myeloma cells and yields additional information for prognosis and can tailor treatment choices for patients. For instance, cytogenetic knowledge has led to better treatment options and outcomes for patients in the use of bortezomib in patients with chromosome 17p deletion (Liu et al 2021) or the use of venetoclax for patients with the known chromosomal translocation t(11;14) (Basali et al, 2020).
Treatment overview
Myeloma is a complex blood cancer and although it remains incurable, advances in therapies have provided patients with better overall survival and longer durations of remission. Treatments for myeloma have changed dramatically. The development and increasing numbers of active agents have generated numerous possible drug combinations that can be used in first-line therapies, patients eligible for transplant and those who have relapsed.
The three main classes of drugs for the treatment of myeloma are:
- Proteasome inhibitors
- Immunomodulatory agents
- Monoclonal antibodies (mAbs) (Mikhael, 2020).
However, many patients become refractory to all three of the major classes of myeloma treatment and alternative treatment options are needed. Antibody-drug conjugates such as belantamab and targeted therapies for specific translocations such as venetoclax for t(11:14) are available and in some cases are reimbursed but may not always be accessible, depending on the location of the treatment centre. As a result of the DREAM III study where belantamab monotherapy was compared with pomalidomide and low-dose dexamethasone in patients with relapsed disease, belantamab was withdrawn for use in the relapsed setting due to this study not meeting its primary end points of a progression-free survival benefit (Ryan, 2022).
Immune-based therapies such as CAR-T and bispecific therapies such as teclistamab provide exciting new options for patients who have become refractory to triple-class drug combinations. However, availability and sometimes funding may inhibit the treatments made available to patients. Other advances have provided hope for patients but they also result in additional and unfamiliar side effects for patients and their families. Specialist nurses working in haematology need knowledge of these side effects in order to ensure they educate patients and families and can respond effectively to adverse events.
Newer treatment options for myeloma and nursing considerations are outlined in Table 1.
Table 1. Newer treatments: symptom challenges and nursing considerations
| Treatment | Important nursing considerations |
|---|---|
| Daratumumab A monoclonal antibody targeting CD38. CD38 is a protein highly expressed on the surface of myeloma cells |
|
| Ixazomib A second-generation proteasome inhibitorMyeloma cells are particularly sensitive to proteasome inhibition. When their protein recycling system is shut down myeloma cells die |
|
| Carfilzomib A second-generation proteasome inhibitor |
|
| Venetoclax An oral BCL-2 inhibitor that induces cell death in myeloma cells, especially in patients with chromosomal translocation t(11;14) |
|
| Belantumab mafodotin An anti-B-cell maturation antigen (BCMA) antibody-drug conjugate (ADC) |
|
| Selinexor An oral drug and first-in-class selective inhibitor of nuclear transport (SINE). This compound. inhibits the protein XPO1, involved in reactivating tumour-suppressing proteins and inducing tumour cell apoptosis |
|
| Teclistamab A human bispecific monoclonal antibody targeting both CD3 on T-cells and B-cell maturation on plasma cells |
|
| CAR-T therapy A patient's own T-cells are collected and genetically engineered so they better recognise and destroy myeloma cells |
|
Newer treatment options in myeloma
Daratumumab
Daratumumab was the first monoclonal antibody approved by the US Food and Drug Administration (FDA) for the treatment of myeloma (Lokhorst et al, 2015). The manufacturers recommend a daratumumab infusion over 3 hours, and reports confirm that most infusion-related reactions occur on the first daratumumab infusion (Geirnaert et al, 2021). However, many centres now use rapid infusion over 90 minutes (after the first two doses of daratumumab) (Hamadeh et al, 2021), which has been shown to be well tolerated and safe (Lombardi et al, 2021).
The results of two recent studies, COLUMBA and PLEIADES, (Mateos et al, 2020; Chari et al, 2021) have informed FDA approval of a new subcutaneous preparation of daratumumab, containing recombinant human hyaluronidase (2000 units/ml).
The COLUMBA study reported comparable clinical efficacy to intravenous daratumumab and an improved safety profile with relapsed and refractory myeloma. Similar findings were reported in the PLEIADES study, which used subcutaneous daratumumab in combination with standard-of-care regimens for newly diagnosed transplant-eligible, transplant-ineligible and relapsed/refractory myeloma (Chari et al, 2021).
Subcutaneous daratumumab reduces administration time (3-5 minutes) (Chari et al, 2021) and patients who receive subcutaneous daratumumab report higher satisfaction with their cancer treatment when compared with patients whose daratumumab is administered via the intravenous route (Usmani et al, 2018). In addition, a recent retrospective observational study reported subcutaneous daratumumab to be well tolerated in a cohort of patients (n=58), including 22 who had not previously received daratumumab, with no patient requiring monitoring or rescue medications at home (diphenhydramine 25 mg and methylprednisolone 20 mg) to manage signs and symptoms of administration-related reactions (Hamadeh et al, 2021). The majority of infusion-related reactions occur on the first daratumumab infusion. A higher infusion reaction rate occurs with intravenous than with subcutaneous routes. Patients who have previously been treated with intravenous daratumumab can be safely switched to the subcutaneous formulation without requiring monitoring or intensification of pre-medications. The importance of subcutaneous daratumumab is most relevant now in the context of COVID-19 and the need to reduce patients' time spent in hospitals and their number of visits (Hamadeh et al, 2021; Perego et al, 2021).
Daratumumab has recently been approved by the National Institute for Health and Care Excellence (NICE) as a four-drug combination treatment for newly diagnosed transplant eligible myeloma (NICE, 2022). This is also the first four-drug combination approved in Ireland and follows the findings of a European trial (CASSIOPEIA) involving 111 centres that showed the clinical benefit of including daratumumab with standard treatment for transplant-eligible patients with newly diagnosed myeloma (Moreau et al, 2019).
Carfilzomib
Carfilzomib is a second-generation proteasome inhibitor (PI) with high selectivity resulting in fewer adverse effects, including peripheral neuropathy (a debilitating effect seen with bortezomib, a first-generation PI) (Jayaweera et al, 2021). Carfilzomib was originally approved as monotherapy. Now, based on results reported in two landmark studies, ASPIRE (Stewart et al, 2015) and ENDEAVOR (Dimopoulos et al, 2016), carfilzomib is also approved in combination with lenalidomide with dexamethasone (Len-Dex) and with dexamethasone for patients with relapsed/refractory myeloma. It is important when administrating carfilzomib that intravenous fluids be given before and after administration to minimise renal toxicity and the risk of tumour lysis syndrome. Additionally, patients should be pre-medicated with dexamethasone to minimise infusion reactions. Moreover, cardiovascular adverse events are linked with carfilzomib. Therefore, a cardiac baseline assessment such as cardiac history, blood pressure, trans-thoracic echocardiography and ECG is recommended (Astarita et al, 2021).
Ixazomib
Ixazomib is also a second-generation proteasome inhibitor and has a similar mechanism of action to bortezomib. Ixazomib is the first oral proteasome inhibitor and is approved for use in more than 50 countries worldwide used in combination with other agents to treat myeloma (Richardson et al, 2018). Ixazomib is particularly valuable in older aged/frail patients due to its oral administration and manageable toxicity profile. Moreover, older aged/frail patients can remain on ixazomib therapy for long time periods and their outcomes are similar to younger patients also on ixazomib-based combinations (Richardson et al, 2018). It is well tolerated as a single agent or in combination; however, patients should be monitored for skin rashes and gastrointestinal toxicity, which tends to occur shortly after commencing the drug. Ixazomib has been described as causing fewer issues with neuropathy compared with bortezomib, which may be something to consider in elderly or frail patients. However, it is associated with a higher risk of zoster reactivation so appropriate prophylaxis adhering to local policies should be observed. Advice should be given on administration with food as food interferes with absorption so a gap of 1 hour before food and 2 hours after should be encouraged.
Venetoclax
Venetoclax offers another novel approach to the treatment of patients with relapsed/refractory myeloma positive for t(11;14) for whom multiple previous therapies have failed (Kumar et al, 2017). Venetoclax is an oral BCL-2 inhibitor therapy that induces cell death in myeloma cells, especially in patients harbouring t(11;14) (Kaufman et al, 2021). The chromosomal translocation t(11;14) is the most frequent translocation in myeloma and is seen in about 15-20% of newly diagnosed patients (Foncesca et al, 2002). The most common adverse effects of venetoclax include infection risk, cytopenias and gastrointestinal side effects. Trial evidence suggests that venetoclax-based therapy should not be used for patients without t(11;14), particularly relapsed refractory myeloma patients who have had many prior treatment lines because these patients have severely compromised immunity and are at high risk of serious infections (Ehsan et al, 2021).
Belantamab mafodotin
Belantamab mafodotin is a first-in-class anti-B-cell maturation antigen (BCMA) antibody-drug conjugate (ADC), granted accelerated approval by the FDA in August 2020 (Lassiter et al, 2021). ADCs work as carriers to bring cytotoxic agents into myeloma cells, resulting in a targeted attack on tumour cells with less toxicity on non-targeted cells. ADCs contain a monoclonal antibody, a linker attaching the drug to the antibody, and a cytotoxic agent (Lassiter et al, 2021). BCMA is expressed on myeloma cells and plays a role in facilitating the long-term survival of plasma cells. Moreover, BCMA is used as a prognostic biomarker in myeloma (Shah et al, 2020). The expression of BCMA can be detected on all CD138+ myeloma cells, but it is not expressed in any other tissues, therefore, due to this receptor specificity, belantamab mafodotin acts only on the malignant myeloma plasma cells, thus resulting in reduced toxicity in non-targeted tissues (Lassiter et al, 2021). Currently indicated in the relapsed or refractory setting, belantamab mafodotin has been shown to cost less and increase quality-adjusted life years when compared with selinexor plus dexamethasone (Nikolaou et al, 2021).
Keraptopathy (damage to the cornea) is a known risk with belantamab mafodotin. As shown in the DREAM-2 trial, patients with a prior history of dry eyes were more likely to develop corneal damage (Ferron-Brady et al, 2020). An ophthalmic examination is recommended prior to and during belantamab therapy. Dosage can be reduced or timing between doses extended if ocular toxicity such as blurred vision, dry eyes or corneal ulceration occurs. Belantamab mafodotin should be discontinued if ocular toxicity is severe (Lassiter et al, 2021). As mentioned previously, the FDA has withdrawn the use of belantamab as a result of the DREAM III trial but other trials are still ongoing.
Selinexor
Selinexor is an oral selective inhibitor of a compound that blocks exportin 1(XPO1). Exportin 1 (XPO1) is overexpressed in a large number of tumours, and in myeloma (Richter et al, 2020). Selinexor has been approved for administration in combination with dexamethasone in the relapsed patient. This was based on the STORM trial. The most common side effects experienced were fatigue, nausea and decreased appetite as well as thrombocytopenia. Up to 20% of patients discontinued therapy due to related adverse events while participating in this trial (Richter et al, 2020).
Teclistamab
This is a T-cell redirecting bispecific antibody that targets both CD3 on the surface of T-cells and B-cells maturation antigen expressed on the surface of myeloma cells (Moreau et al, 2022). The aim of the MajesTEC-1 study was to evaluate the safety and tolerability and efficacy of teclistamab in patients with relapsed or refractory disease (Usmani et al, 2021). The FDA approval comes with a boxed warning for cytokine release syndrome and neurotoxicity. Other common side effects are pyrexia, neutropenia, anaemia and musculoskeletal pain (Moreau et al, 2022). Overall response rates compare favourably with belantamab and are in line with CAR-T cells without needing specialised care centres and a waiting time for CAR-T cell production (ESMO, 2022).
CAR-T cells
CAR-T cells are approved in myeloma that has relapsed or is refractory to at least four prior treatments. It is described as a type of cancer immunotherapy and helps the body's own immune system to find and attack cancer cells. T-cells are extracted from a person's blood using a process called leukopheresis. The T-cells are then frozen and sent to a lab where they are genetically altered so they have specific receptors called chimeric antigen receptors (CAR) on their surface. These receptors help the T-cells to attach to proteins on cancer cells and help the immune system attack them (Lamprecht and Dansereau, 2019). Side effect profiles with CAR-T cells includes cytokine release syndrome, pyrexia, difficulty in breathing, tachycardia and neurological toxicities such as loss of balance or difficulty with understanding and speech (Baer, 2021). The availability of CAR-T cells is limited to specialised centres and it also comes with a financial cost as described previously.
Side effect profile and the nurse's role
The introduction of many new potent anti-myeloma agents has introduced more complexity to the treatment decision process. The standard has shifted from short-term drug exposure to long-term treatments, and awareness of early and late drug toxicities has become increasingly important (Delforge and Lundwig, 2017). Side effect profiles associated with myeloma therapies are vast because treatments are often integrated with different combinations of drugs to obtain the best possible results and better progression-free survival. It can be difficult to isolate which side effects are associated with which drug or if the side effects are associated with the underlying disease. Therefore, treatments for patients should be tailored specifically not only to disease characteristics but also to patient factors such as age, general condition, comorbidities and side effects experienced by previous therapies. In addition, screening for risk factors, regular monitoring and the early recognition of side effects can mean that side effects can be managed at an early stage. This subsequently leads to increased patient adherence and continuing therapy until disease progression, which is paramount when treating patients with myeloma.
However, as newer therapies and drug combinations become more available, some misunderstanding has developed regarding the choice of drugs being used for initial therapy, the role of transplant, and the role of maintenance therapy (Yang et al, 2020). In addition, drug availability, approval, reimbursement of cost, and accessibility will have an impact on patients' choices. More importantly, the choices considered for patients must also include a transparent conversation regarding the long-term value and the impact of continuous long-term effects on the individual's quality of life and daily activities (Janssens et al, 2021). A recent qualitative study with myeloma patients (n=22), revealed their concerns regarding adverse effects of continuous treatment such as permanent organ damage, bone fractures and debilitating neuropathic effects, which patients felt reduced their independence and mobility. Patients also expressed concerns about the effect of treatment on their cognitive function, susceptibility to infection, reduced energy, pain and emotional issues (Janssens et al, 2021).
Age continues to be a factor in treatment decision-making as it weighs heavily in most frailty tools, which often restrict older patients from clinical trials. However, age alone is insufficient to guide treatment choices (Pawlyn et al, 2022). Developments in older people's fitness and ability to tolerate myeloma therapy are gaining attention, with improved tools emerging that allow for the assessment of biological rather than chronological ageing (Möller et al, 2021). In addition, a multidisciplinary clinic managed by a doctor, nurse, and physiotherapist has shown significant improvements in myeloma patients' (n=61) exercise scores, with 83% feeling more confident in self-management (Lecat et al, 2023).
Nurses play a central role as part of the multidisciplinary team supporting myeloma patients and their carers on their long treatment journey punctured with relapses and remissions. This support is increasingly needed with the addition of new treatments for myeloma.
Nurses now have a range of patient-reported outcome measures (PROMs) validated for routine practice that can be used to assess myeloma patients for global quality of life (QoL) symptoms and supportive care needs (King et al, 2017). These include the Myeloma Patient Outcome Scale (MyPOS) (Osborne et al, 2015), the Haematology Information Needs Questionnaire (HINQ-62) (Rood et al, 2018) and the HM-PRO (Goswami et al, 2020). The MyPOS uses a 5-point Likert scale to assess 13 symptoms and 20 QoL items experienced in the past week. The 62-item HINQ also uses a Likert scale (6 points) and the core areas of assessment are disease, symptoms, treatment and side-effects; aetiology, sleep and physical changes; self-care; medical tests and prognosis; and psychosocial (Rood et al, 2018). The HM-PRO consists of two independent 3-point Likert scales, one measuring impact on health-related QoL using 24 items and the other measuring 18 items related to signs and symptoms (Goswami et al, 2020). However, despite growing evidence to support the use of myeloma-specific PROMs, they are not being used in standard care across UK haematology centres (Kirkpatrick et al, 2023).
Conclusion
With increasing knowledge of myeloma and the changes and combinations in treatments, patients are surviving longer. More exposure to various different treatment types has helped patients, families and experts treating the disease. However, it also can carry the risk of having to manage more long-term and sometimes debilitating side effects related to these treatments. There is a need for unambiguous communication with myeloma patients about treatment outcomes, drug developments and uncertainties regarding potential long-term effects and safety (Janssens et al, 2021). Nurses are at the forefront of patients' journey and play a central role in supporting patients and families to manage side effects. This means that patients can continue the treatments for as long as possible with the aim of maintaining a good quality of life.
KEY POINTS
- People living with a diagnosis of myeloma are surviving longer due to treatment advances
- The multitude of drug combinations approved for use to treat myeloma has resulted in more long-term and sometimes debilitating side effects
- Nurses need knowledge and skills in recognising and managing side effects associated with newly approved drugs to treat myeloma
- Nurses now have a range of myeloma-specific patient-reported outcome measures (PROMs), such as the Myeloma Patient Outcome Scale (MyPos) and Haematology Information Needs Questionnaire (HINQ-62) for the assessment of patient symptoms and support needs
CPD reflective questions
- What side effects do most patients with myeloma in your practice experience?
- What self-care strategies do you advise to help patients cope with common side effects?
- What are the symptom challenges and nursing considerations with the use of second-generation proteasome inhibitor (PIs) and antibody-drug conjugates in the treatment of myeloma?
- What are the barriers to using myeloma-specific patient-reported outcome measures in routine care and how can these be addressed?