

Hidradenitis suppurativa (HS) is a chronic, inflammatory recurrent debilitating skin disease of the hair follicle that usually presents after puberty with painful, deep-seated, inflamed lesions in the apocrine gland areas of the body, most commonly the axillary, inguinal and anogenital regions (Saunte and Jemec, 2017) (Figure 1). Globally reported prevalence in western populations is 1%, with a range of 0.03-4%, including probable cases, although this figure may often be inaccurate due to failure to diagnose or misdiagnosis. Disease progression can be unpredictable and usually lasts until about 60 years of age; it affects both adults and children and has a female to male ratio of 3:1 (Ingram, 2020). Aetiology is still unclear, making identification difficult, which leads to delays in diagnosis or mismanagement. This results in complications with more severe disease or comorbidities, as well as wound chronicity (Kokolakis et al, 2020).
Diagnosing the condition
Painful chronic wounds appear with discharge, odour, and complications such as infection and tunnelling, which can lead to scarring and disfigurement (Figure 2). Often reduced mobility and physical disability ensue as a result of distorted skin. Additionally, periwound skin may become macerated and excoriated in the presence of mismanaged exudate, and patients are at risk of adhesive-related skin injury (Figure 3). Relentless duration of physical symptoms, associated restrictions in daily living and frustration combine to contribute to feelings of overwhelming fatigue.


Diagnosing HS is relatively straightforward. A simple algorithm was developed in 2014 (Vinding et al, 2014). It calls for two questions to be asked of the patient:
- Have you had an outbreak of boils in the past 6 months?
- If yes, how many outbreaks, and in what locations?
Two or more outbreaks in the axilla, breasts, buttocks, groin or genital regions can be diagnosed as HS with more than 90% specificity and accuracy, and the patient should be referred to dermatology.
Once a diagnosis has been confirmed, severity needs to be established in order to implement the correct treatment and monitor ongoing management because, unfortunately, diagnostic delay remains significant. In 2018, in Ireland Delany et al (2018) reported delays of up to 8.5 years, and more recent global data show that they have grown even longer, currently standing at 10.2 years (Garg et al, 2020; Kokolakis et al, 2020).
The Hurley scale, developed in 1989 to describe the severity of symptoms, has been validated, updated and refined several times, most recently in 2019 to include extra detailed staging (Hurley, 1989; Prens et al, 2019; Ovadja et al, 2019). However, I would add that awareness of the disease is lacking: as von der Werth (2001) put it, ‘To diagnosis HS, one has to first and foremost think of it’.
My HS story
The first symptoms appeared when I was about 12 or 13 years old, although I hid my symptoms due to embarrassment and shame until I was 17 years old when I was taken to see a GP who treated me with antibiotics for skin infection and abscesses. Antibiotic treatment continued until I was 20 years old when I underwent surgery to excise the lesions. However, I remained undiagnosed, and the lesions worsened and spread to new locations. I was then referred to a colorectal surgeon as it was thought that it was Crohn's disease.
Following a wide excision around the perianal area, I remained undiagnosed until further surgery and investigations at the age of 23 when the surgeon ruled out Crohn's disease. Finally, I was diagnosed with HS and referred to dermatology. This was a bittersweet moment, because I could finally put a name to my condition. However, I quickly discovered that it is incurable. Symptoms can be reduced with robust therapeutics and surgery, but the disease recurs—it can be controlled, but no cases of long-term remission have been documented.
I learnt that I would have to deal with these wounds and lesions, and other symptoms, such as malaise and fatigue, for the rest of my life. Over the years, I have had 13 surgeries and a range of pharmaceutical treatments, many of which are described in the NHS guidelines (NHS website, 2019).
Pharmaceutical interventions
Short- and long-term antibiotics in various combinations, including intravenous (IV) preparations, were prescribed to treat or prevent infections. These entailed multiple trips to hospital almost annually and included the administration of IV ertapenem, requiring a peripherally inserted central catheter (PICC) line. Intralesional steroid injections and hormone therapy with androgen blockers were given to interrupt the progress of the lesions. Evidence exists to support treatment with metformin for common dermatological conditions such as acne, pemphigoid disorders and HS, and research has indicated that adalimumab creates antibodies against tumour necrosis factor alpha (Badr et al, 2013; Kimball et al, 2016).
All of these interventions have been tried, but failed, to prevent recurrent flare-ups. I am on a high dose of adalimumab at present and, although my symptoms are less severe, I still experience significant flare-ups.
Diary of HS flare
Day 1
The onset begins with fatigue and malaise. The area is a little sore, warm, and tender, and by evening it is swelling and hot to the touch (Figure 4).
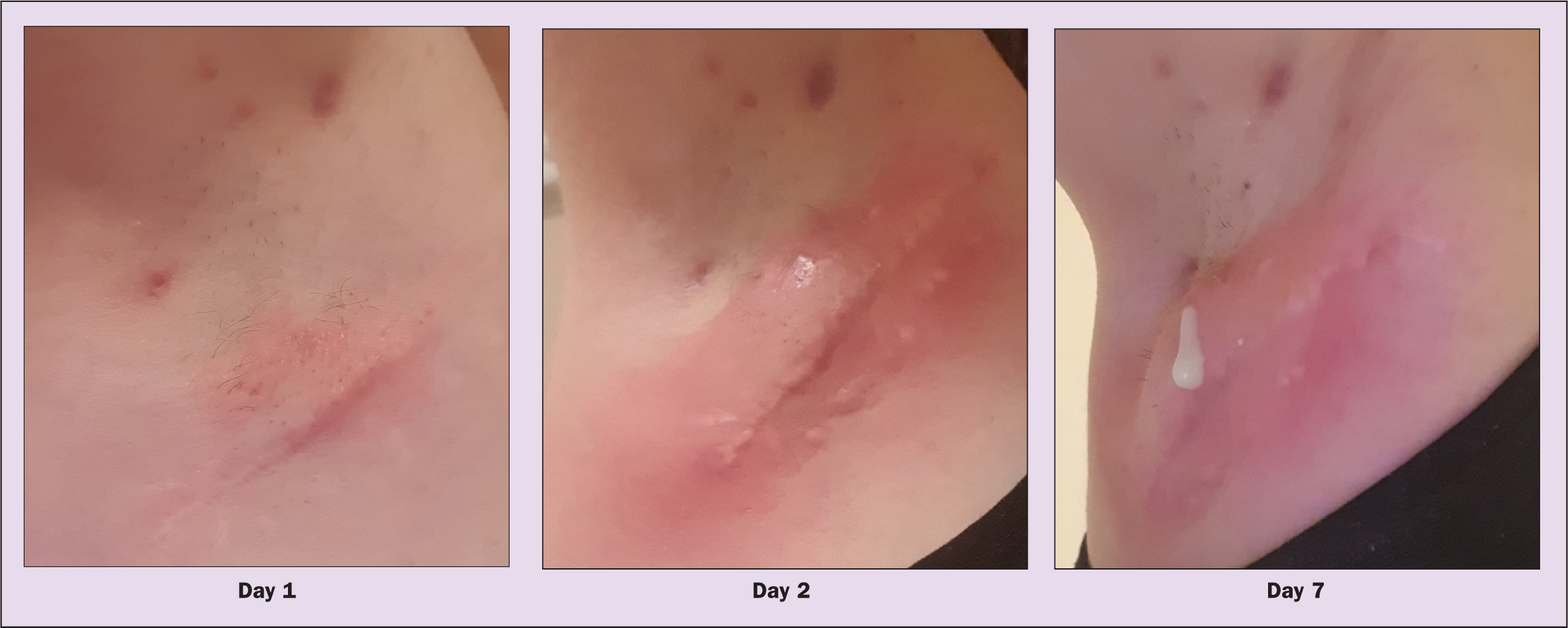
Day 2
The area becomes more inflamed and painful, affecting mobility as the skin becomes stretched and tight. This will usually continue for several days (Figure 4).
Day 7–8
An opening will appear in the skin, causing the lesion to drain, with sinus tracks that continue to trickle and drain beneath the skin (Figure 4). This can continue for weeks, months or even years, depending on the flare-up. It is truly an awful experience. This is just my experience of a HS flare—it may be different for other patients.
In the aftermath of an HS flare-up areas of the skin are left scarred, pitted and disfigured, while the damaged skin tries to heal. This results in pain and restricted movement affecting clothing choices, especially because regular drainage requires management that includes frequently applied, effective wound care with dressings that remain in place.
The biggest challenge is everyday wound care
Adhesive dressings pinch the skin, move about and often fall off, making them difficult to apply, adjust and remove. Additionally, mechanical skin stripping caused by harsh adhesives is a common issue, in which the periwound area becomes compromised due to excess fluid and irritation. In contrast to adhesive dressings, non-adhesive dressings have the propensity to become displaced or bunched, causing skin damage through additional pressure or leaks if exudate is not adequately managed.
From a personal perspective, bulky dressings can be indiscreet and embarrassing, as well as restrict movement. Frequent dressing changes also add to the embarrassment and inconvenience experienced as part of daily living.
HS patient survey
A survey of 908 people from 28 countries was conducted by the author and published last year (Moloney et al, 2021), with women making up 95% of the sample; 85% of the respondents were aged 25-54 years. The survey aimed to establish the impact of HS on patients' quality of life and their experiences of managing their condition with available wound-care regimens. In 81% of cases, respondents reported experiencing a negative impact on quality of life due to frequent dressing changes; 16% required five or more dressing changes a day and 12% had to spend more than 30 minutes a day on their wound care. Unsurprisingly, 81% reported experiencing pain during the dressing changes and there was an overall dissatisfaction with currently available wound dressings.
Patient-reported experience
Typical comments included:
- ‘I need assistance for application in areas that are hard to reach due to pain of the movement. The removal of the bandages is uncomfortable and tears my skin’
- ‘It's embarrassing to ask others to apply dressings’
- ‘It's a never-ending issue. Relationships ended due to dressing wounds all the time. It's depressing that others don't understand the frustration of wounds not healing or reopening, causing depression and suicidal thoughts’
- ‘I feel alone and isolated, constantly worrying about leaking, smell, dressings falling off. It has impacted every aspect of my life, to the extent that I really have no life.’
Embarrassment and shame, stress and anxiety were commonly experienced with regard to the stains and odour associated with failure to manage exudate.
Impact on work life and emotions
Respondents described their experiences at work: ‘Work is the worst. It is uncomfortable and I worry about the smell. I have to steal away in an upstairs toilet where the main door locks so I can use the mirror. Depending on the flare-up, this can be for 5-10 minutes around 3-4 times during the working day.’
Their home life was equally challenging: ‘Relationships with my children are affected. I am unable to join in all the games, to hold them, they can't sit on my lap. I am watching them grow from the sidelines.’
Dressing requirements for HS
The majority of patients reported requiring dressings for more than 6 months of the year, with an average of 2.8 dressings changes a day. Patients reported spending a considerable time managing their wounds. Adhesive dressings were the most commonly used option and, incredibly, 44% of respondents used improvised dressings that comprised kitchen roll, toilet paper or hygiene products (Moloney et al, 2021).
The solution
Criteria for the ideal wound dressing system for hidradenitis suppurativa
- Kind to skin: does not damage wound or surrounding skin
- Highly absorbent: can contain large volumes of exudate
- Secure retention: reduces slippage, chafing and leaks
- Soft and gentle: flexible and body conforming
- Easy to use: easy to apply, adjust and remove
- Adhesive free: non-adhesive or gentle adhesion, if required.
HidraWear
Exasperated, I decided to create a wound-management approach that would work for me and for others living with HS. I founded a company called HidraMed Solutions with a mission to design and develop viable and acceptable wound-care solutions to manage HS and difficult-to-dress areas of the body that would allow patients to self-manage their wound-care regimen. This has resulted in the development of HidraWear wearable wound care, which sits at the intersection of home care and health care.
The system comprises a flexible absorbent dressing to manage exudate in difficult-to-reach areas and is held in place within soft garments that look like regular clothing. The dressing is placed inside the garment under specially designed perforations. The back of the dressing has a customised loop coating that allows the fastener to adhere to it through the perforations. The fastener is then placed on the outside of the garment on the footprint of the dressing. The dressing is secured in place through a hook and loop mechanism without the use of adhesives (Figure 5).

Challenges
Correct diagnosis is the first step to providing an effective solution, taking account of the severity rating in each individual case using the simple, reliable Hurley scoring tool, which classifies HS severity into: stage 1 (mild), stage 2 (moderate) and stage 3 (severe). This will ensure appropriate wound management at each stage of severity.
Although many studies have yielded innovations in pharmaceutical interventions, standard practice is limited, and few guidelines focus on best practice in wound care in the context of HS, with scant reference to viable management options (Smith et al, 2018). The presence of highly exuding wounds in difficult-to-reach, warm and moist areas of the body present challenges when using currently available wound-management products, especially because adhesive dressings may cause skin stripping and non-adhesive dressings may become displaced, causing similar skin trauma.
Challenges with wound-care provision are compounded by the paucity of evidence to highlight the availability of effective, yet tolerable, solutions that consider each patient as an individual. Standard treatment for managing highly exuding wounds may not cope with the constant draining of fluid from tracking sinuses, and the problem of keeping dressings in place where heat, hair and moisture may challenge fixation for long periods of time.
As the responses to the survey showed, other sufferers fared no better than I did, with some resorting to non-medical padding, such as sanitary towels or toilet paper, to mop up the discharge. Mobility is often hampered by stiff, scarred skin or bulky wound-care regimens. Therefore, self-care solutions such as HidraWear, which incorporate the dressings into clothing similar to regular everyday wear and allow flexibility of movement during daily activities, can help manage exudate effectively even with frequent dressing changes, and could minimise the feelings of anxiety and stress.
Conclusion
Each patient is an individual and currently available treatments do not adequately consider the complexity of HS, the recurrence of flare-ups and the difficulty of managing frequent dressing changes in awkward anatomical areas that are often painful and sensitive.
As a result of my experiences of living with HS and my frustrations with each failed attempt at a practical wound-care solution, I was grateful for the opportunity to design a simple wound-care regimen. Thankfully, it fulfils all the criteria to manage exudate and incorporates a safe, gentle method of keeping the dressings in place. This has finally given me the chance to move forward with my life and provide a glimmer of hope to fellow sufferers. It enables me, and others with HS, to self-manage my wounds in the home setting and gives me a sense of control over my disease and my life.
There is still a long way to go before HS is more widely recognised and its management receives the attention from those involved in developing solutions and providing wound care that those with HS deserve. Combining awareness of the condition, its prevalence in the community and a relatively simple diagnosis pathway with appropriate HS-specific treatment guidelines will almost certainly lead to a meaningful improvement in the lives of this underserved, highly distressed and sadly oft-overlooked patient group..
KEY POINTS
- Hidradenitis suppurativa (HS) is an inflammatory skin condition presenting with painful, exuding lesions that lead to scarring and mobility restrictions
- HS is under-reported, poorly understood, frequently misdiagnosed, and often mismanaged
- Effective wound-care provision and evidence to guide management are limited
- Frequent dressing changes, leakage, odour and appearance can lead to embarrassment and anxiety
- A new regimen addresses the challenges of exudate handling and keeping dressings in place without skin trauma, allowing sufferers to self-care and achieve a better quality of life
CPD reflective questions
- When should you consider a diagnosis of hidradenitis suppurativa?
- What are the most common areas affected by hidradenitis suppurativa?
- How will you decide on and monitor effective wound management?
- How will you support your patients physically and emotionally in managing their condition?