

Challenges with care provision in the community have been acknowledged by national bodies who recognise that district nurses face greater workloads during what is described as a national crisis (Campbell, 2018). Although a joint policy document by the Royal College of Nursing (RCN) and the Queen's Nursing Institute (QNI) (Fanning, 2019) set out a vision for more nursing care to be delivered in the community, district nursing shortages in England were compounded by a 51% increase in nurses leaving between 2013 and 2017. This resulted in around 4000 district nurses caring for a population of approximately 55.8 million in England alone (Fanning, 2019). The situation has been exacerbated by the COVID-19 pandemic, with district nurses and prescribers expressing concern about increasing workloads as patients are discharged early into the community to free acute beds (Penfold, 2020).
The provision of comprehensive clinically effective, yet also cost-effective, wound care is beset with challenges due to rising numbers of patients with chronic conditions and associated wounds (Guest et al, 2015; 2017; Martinengo et al, 2019). Disturbingly, revised data on wounds have shown an increased prevalence of 71% between 2012/2013 and 2017/2018, with a 2% increase in those younger than 65 years of age (Guest, 2021). With the rising number of wounds, concerns have been expressed about increased use of antimicrobial dressings, despite the lack of adequate evidence to support their use for routine wound care (Kramer et al, 2018). NHS expenditure for antimicrobial therapy across the UK rose to £28 million between 2017 and 2018 and analysis by Hussey et al (2019) showed that the use of routine prescribing data to evaluate treatment decisions could have an impact on procurement practice to increase value and reduce waste.
Suboptimal assessment has also been cited as a cause for delays in appropriate treatment and wound healing due to inaccurate diagnosis, correlating with a study by Guest (2021). Guest et al (2021) reported a lack of diagnosis in 25% of all wounds, reinforcing the need for training to assess and devise wound management programmes to provide patient satisfaction with available resources.
Service improvement project: reasons for change
The aim of the project at South Warwickshire University NHS Foundation Trust was to ensure that changes in the wound care service would provide wound management that considered foremost patient outcome, the right dressing in the right time frame and quantity, and reduce the demand on community prescribers. Taking this approach would also release capacity within community services.
Delays in appropriate treatment and wastage
Delays in patients receiving prescribed dressings increased due to the numbers of NHS personnel leaving the service and this has been further exacerbated by staff having to shield due to COVID-19 infection or contact tracing. To overcome clinician shortages, the emergence of supported self-care with correct assessment, appropriate training and prompt access to dressing products is proving to be an important part of providing effective wound management. Problems with patient-specific prescribing have been identified in one NHS trust where delays of up 10 days were reported (Markey and Barrett, 2017). Dressings held in patients' homes may present storage challenges for patients and mean staff may not be able to accurately monitor stock levels. Also, wastage occurs as a result of dressings being discarded when they have been in a patient's home but are no longer needed (Tomes and Dowley, 2022).
Training programmes
The National Wound Care Strategy Programme (NWCSP) has been working on useful guidelines focusing on training to encourage collaborative working with all stakeholders, including industry partners, to improve service delivery to patients (Adderley, 2019). At national level, the RCN and QNI have acknowledged challenges that district nurses face due to declining numbers, detailing the NHS Long Term Plan (2019) to meet the needs of patients while advocating integrated care delivery to support clinicians and maintain a sustainable service (Fanning, 2019).
Since 2020, costs have soared and resources for wound care have decreased as staff have been redeployed to cover management of COVID-19-related conditions, leading to many new initiatives to improve wound care provision. One example of innovation has been the use of paramedics trained by industry to administer minor wound care on-site in the community, using a structured skin tear management pathway with standardised wound dressings, supported by a rigorous training programme. Cost implications were considered alongside the more important aspect of patient needs, because on-site wound management negates anxiety-inducing visits to hospitals and unnecessary delays in treatment (Hickey and Ayres, 2021). A similar project has been rolled out in South Warwickshire, training residential care staff to manage skin tears, with referral to district nurses only needed if a wound does not show signs of healing. This improves patient outcomes, reducing non-scheduled visits for the community services releasing capacity and also reducing paramedic call outs (Mangan and Shoreman, 2021).
Compliance with governance
In an attempt to overcome challenges with supply and wastage, inappropriate past practices such as sharing dressings between patients and keeping dressing stocks in car boots were sometimes in operation, to ensure dressings were readily available for changing conditions (Grothier, 2013).
On the other hand, measures to reduce the numbers of dressings by limiting formularies may result in choice of treatment relying on dressings that are listed but not necessarily appropriate. As the NWCSP works alongside industry to streamline wound dressing usage, the complexity of wound aetiologies and tissue types may also need to be considered to include more comprehensive lists from which to select the most appropriate dressing for individual patients (Brassington et al, 2015). Tissue viability specialists have also highlighted the need for training on dressing materials and an understanding of how they work to ensure that patients' clinical needs are considered ahead of simple cost outlay (Harding and Cutting, 2019).
Audit and identifying areas for improvement
Although the Trust's hospital sites serve the south of Warwickshire, it provides community-based services across the county, covering a population of 569 000. A 2016 audit revealed 711 patients with a wound, of whom 18 patients had multiple wounds, representing a total of 736 wounds. The wound care audit was undertaken across 12 community nursing teams over a period of 1 month, collecting data on all patients being treated for a wound. It recorded type of wound, duration from onset, current treatment, length of visit, and how many visits per week.
Wound duration and dressing changes
Wound duration varied from less than 6 weeks for 33.7% to greater than 12 months for 26% of wounds, with twice-weekly dressing changes taking place in 48.0% and weekly changes in 21.6% of cases (Figure 1).

The total number of dressings used for the 736 wounds was 1553, equating to 2.1 dressings per wound. In all, 93 different products were used, across 23 different categories, in 324 combinations; 50% of wounds had two different dressings and 11.1% had four different dressings per wound. Antimicrobial dressings accounted for 12.8% of those used, although 45.1% of wounds had no signs of infection.
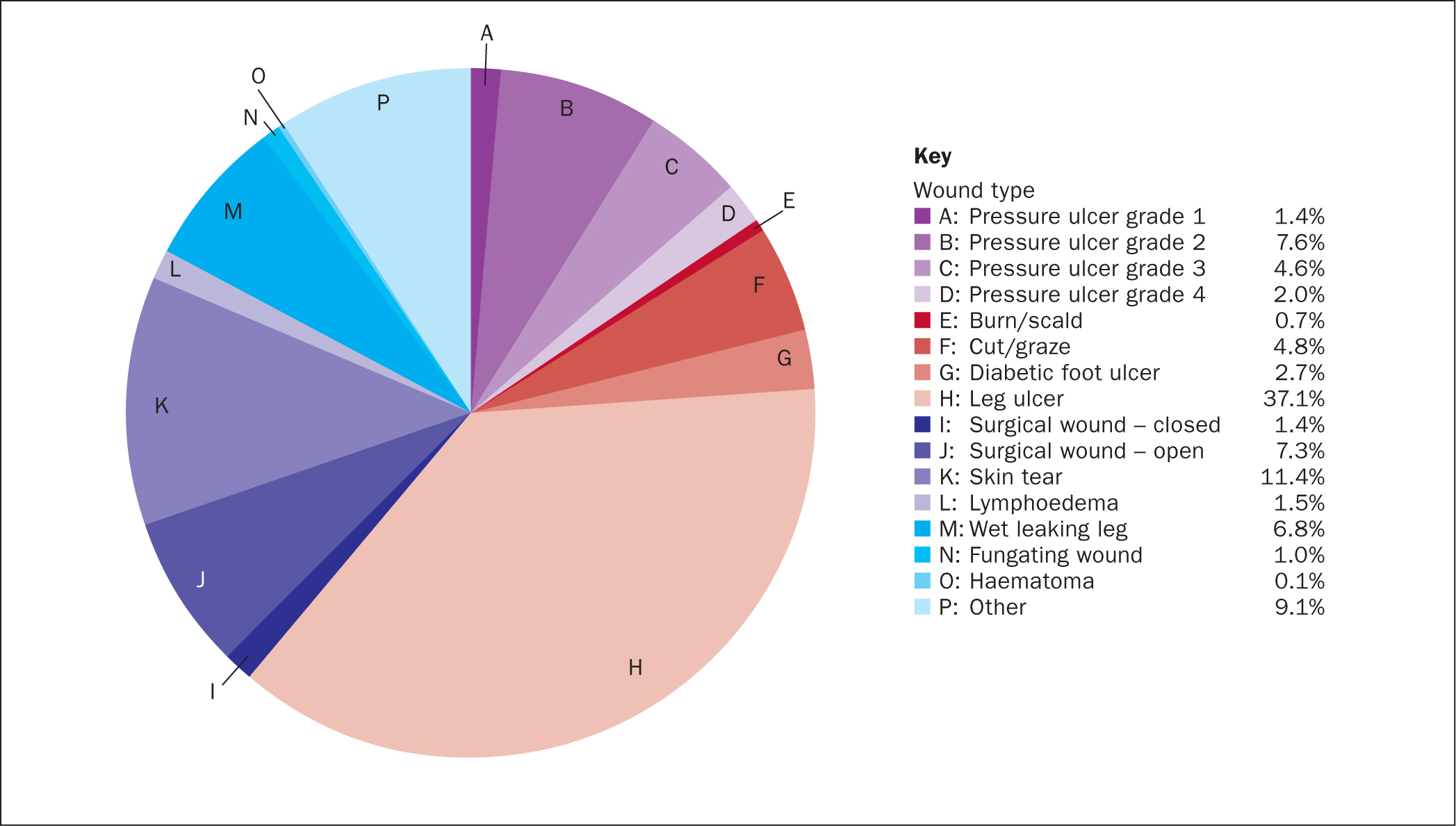
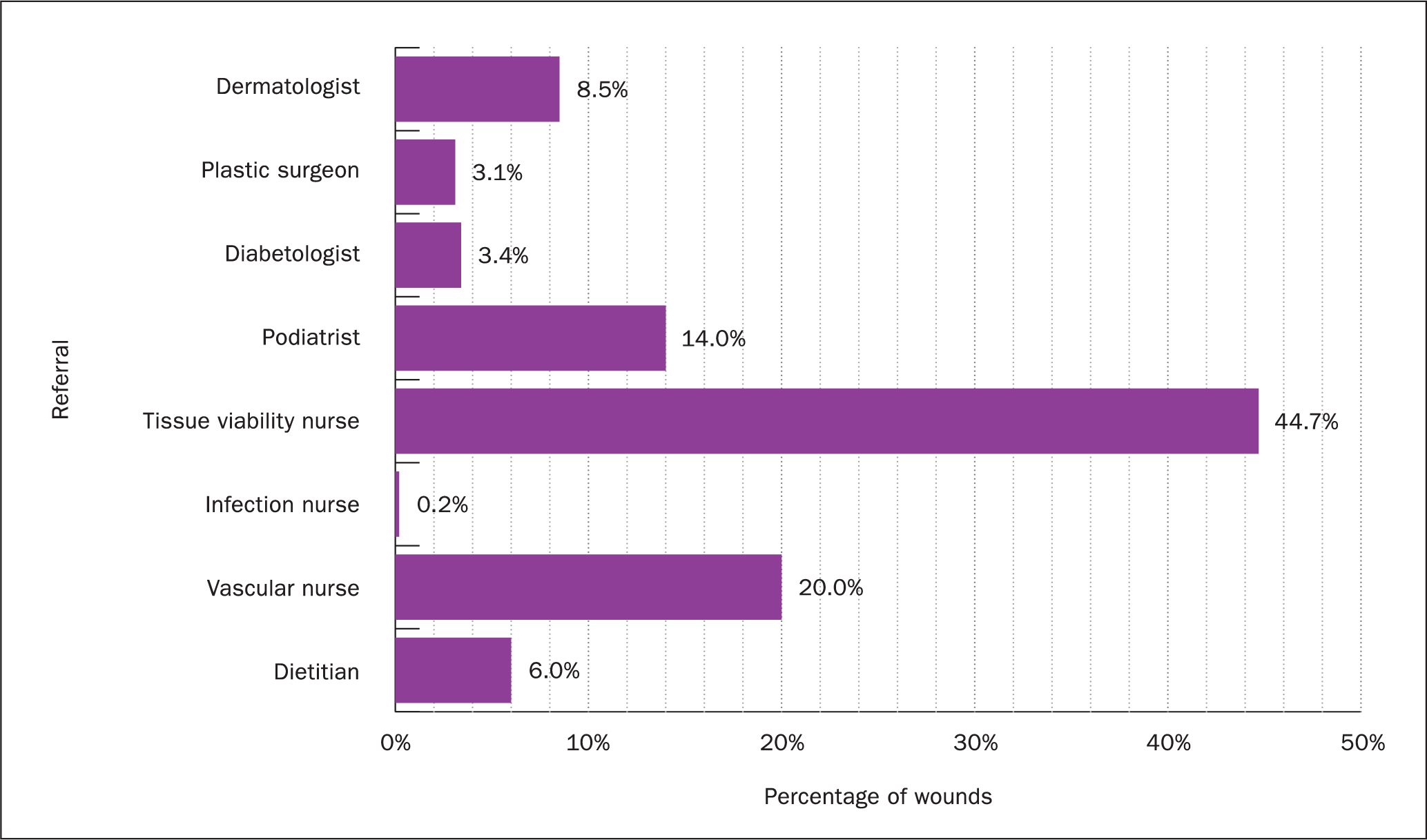
Provision of care
Conditions treated were: 37.0% leg ulcers, 11.4% skin tears, 1.5% lymphoedema, 6.8% wet leaking legs and 15.8% grade 1-4 pressure ulcers, mostly grade 2 (Figure 2). Most of the referrals to the service were from tissue viability nurses, at 44%; other specialties included: 20% of referrals from vascular nurses, 14% from podiatrists and 8.5% from dermatologists (Figure 3). The service was provided by 400 staff and the audit revealed that approximately half of these visits would be for patients with hard-to-heal wounds, not taking into account acute and hospital discharge patients. Only 20% of patients had had one or more admission to hospital, the remaining 80% were cared for in the community.
Patients were managed and visited by registered nurses in 74% of the dressing changes recorded, and another 14% were visited by healthcare assistants; notes for the remaining 12% of changes did not indicate who had applied the dressing. A single patient visit can take up to 1.5 hours of travel time due the extensive reach of the Trust's catchment area.
Changes to the service
A business case that had been originally submitted in 2016 was resubmitted in March 2020 as part of a 4-week master's level leadership course. The business case was approved for roll-out across the Trust covering 12 bases and aligned to a new formulary launch. Formulary compliance was already at 94% and therefore not a key driver. The Gant chart in Table 1 indicates the timeline for the changes.
Table 1. Timeline for service changes
| 2020 | March | April | |||
|---|---|---|---|---|---|
| Week 4 | Week 1 | Week 2 | Week 3 | Week 4 | |
| Business case approval | |||||
| Community nursing team bases identified | |||||
| Locations listed on ONPOS | |||||
| Formulary listing confirmed | |||||
| Confirmation of requisition points | |||||
| Login details created | |||||
| Internal communication sent out | |||||
| First stock order placed | |||||
| Usage data and forecasting confirmation | |||||
| Virtual training of all bases | |||||
| Go live | |||||
| First online order for bases | |||||
ONPOS=Online Non-Prescription Ordering Service
Supply and delivery of wound management
The Online Non-Prescription Ordering Service (ONPOS) was first introduced by Coloplast in 2004 to simplify the prescribing process of wound dressings, reducing wastage and, at the same time, inspiring confidence that patients would receive the right dressing at the right time. The ability to monitor usage provides real-time data on successful treatments and cost outputs, while encouraging formulary compliance and implementing clinically effective wound management. (Grothier, 2013; Griffin, 2015; Jones, 2020). In addition, ONPOS data capture showing reduction in dressings can be used to monitor successful treatment and training programmes to demonstrate evidence-based practice (Mahoney and Simmonds, 2020). The system is used by more than 80 NHS organisations and processes transactions amounting to £21 million each year. With more than 300 orders per day, it supports three supply routes: NHS Supply Chain, local pharmacies and wholesalers (Jones, 2020).
Training and effective use of technology to reduce risk and spend
A review of training services identified successful partnerships with industry to provide bespoke programmes, designed to deliver training in clinical governance, wound management and supply routes. Over the 3-month total implementation period, systems were set in place to ensure good communication with staff, providing support for the project and enabling them to understand their roles and responsibilities. This included training in a level 4 programme to manage major incidents.
All teams had an allocation of three people to manage the ONPOS/direct supply with training in the use of ONPOS set up in conjunction with Coloplast. Order numbers were provided and store cupboards were prepared in the team base locations to receive the stock. Sufficient stock for 1 month was ordered for each team based on the previous year's prescribing and made available in store cupboards.
Fortnightly virtual team meetings were held to support change, with tissue viability nurses receiving emails asking for feedback regarding concerns. At this point wound care prescribing by district nurses was stopped and a company representative was sent out to all bases to support, advise and resolve any issues to ensure a positive outcome with the non-prescription ordering system.
Impact of changes
Comparison of the NHS financial year 2019/20 with 2020/21 and 2021/22 showed savings of approximately 29% as a result of moving from patient-specific prescribing to centrally held stocks, thereby surpassing the initial cost-neutral aim. The process was also much simpler and quicker, meaning that patients did not suffer from unnecessary delays in receiving the dressings.
An additional step taken was the Trust ‘bagging up’ 1 months' worth of stock per patient to reduce the footfall into patients' homes and coming back into the office during the pandemic. This was then reduced to 2 weeks' worth once teams were allowed back into the office in larger numbers.
One challenge was the use of qualified nurses within some teams to monitor stock levels and put away dressings. The financial savings achieved have allowed the tissue viability nurse leads to submit a business case to employ three additional staff to support the use of non-prescription dressings, and to provide a more sustainable service moving forward. This would release nurses to concentrate on hands-on wound care, based on structured pathways and supported by a well-run dressing supply service.
Table 2 summarises the outcomes identified. Feedback from nurses was positive:
‘We always have stock available for patients.’
‘Prior to ONPOS, it would take a long time to receive a prescription as we only had two prescribers.’
‘It's quicker to get a patient on the required care plan.’
‘The system is really easy to use.’
‘Patients can start the correct care plan straight away and change their current care plan quicker.’
Table 2. Outcomes of service improvement project
| Practitioner | Patient | Trust |
|---|---|---|
| Evidence-based practice and training to provide safe, effective wound care despite staff shortages. Reduce the risk of litigation and the length of time from assessment to the patient receiving the dressings | Improved quality of care and reassurance of timely, appropriate and safe care | Reduction of economic costs by reducing dressing wastage. Alignment to governance through training and effective wound care practice |
Discussion
Despite nurse shortages and rising numbers of patients requiring care, community nurses continue to provide essential care, ensuring that changes in practice do not fail patients (Penfold, 2020). Value-based procurement in wound care was discussed by Posnett (2022), who cautioned against the practice of cost-containment measures that consider unit costs of dressings without including nurse time and overall healing, which may lead to short-term gains to the detriment of long-term outcomes. He advised decision-making that achieves better patient and cost outcomes with available resources or the same outcomes with lower resources. An example of total cost calculations using different dressings demonstrated savings that can be made by taking into account unit costs, nurse time, time to healing and adjunct costs associated with dressing changes. This type of practice relies on training and education to make informed decisions (Posnett, 2022).
During and following the COVID-19 pandemic, formal education programmes were disrupted while nurses coped with providing the same level of care in an environment where more patients fell into high-risk categories and chronic conditions deteriorated due to delays in referrals. Web-based meetings and online resources have become an important platform for learning and education.
Alongside training programmes, industry has stepped up to provide service delivery of dressings that negates the need for community nurse prescribers while still involving community pharmacists. Online non-prescription systems such as the well-established ONPOS system have revolutionised dressing supply services, with measurable reduction in costs and time-consuming processes associated with previous practice. Similar successful practice has been recorded in areas such as Central Essex, Powys, Brighton and Hove and Wolverhampton (Grothier, 2013; Griffin, 2015; Jones, 2020; Tomes and Dowley, 2022). Tomes and Dowley (2022) discussed how initial fears of deskilling prescribing staff in one Trust were allayed with successful implementation.
As South Warwickshire University NHS Foundation Trust had been forward-thinking even before the pandemic by going paperless and using advanced technology with up-to-date laptops, systems were already in place to move seamlessly into a new way to cope with the changing world of working safely in the community. Auditing the service identified resources and stock levels that are maintained using the ONPOS to record real-time data and ensure adequate dressings without wastage, and additional patient benefits, with the addition of stock takers, releasing experienced staff for patient management.
Practical and electronic ongoing support is vital to the success of this new way of working in the community to ensure smooth running and patient benefits with improved healing and good clinical practice in the context of uncertainty around COVID-19 and staff shortages.
Conclusion
Patient care was increased by addressing a financial and resource need aligned to the National Wound Care Strategy and maintaining 100% formulary compliance. Adopting the ‘patient first’ approach with auditing, education and a wise use of available resources and budget has achieved optimum clinical, patient and financial outcomes, with data for 2021/2022 recording savings that have been sustained over the past 2 years.
KEY POINTS
- Audit is required to identify areas for improvements and the judicious deployment of resources
- Industry plays an important role in training and service delivery
- The use of an online non-prescription ordering system for dressings streamlined the service and reduced overall wound care spend
CPD reflective questions
- How often do you audit your service? Do you think that this is the appropriate frequency?
- In your team/workplace, who decides on changes to training and resource management and how easy is it to change practice?
- Are there facilities to implement web-based training in your workplace?
- In your team/workplace, what is the preferred method of supplying dressings?