References
Introducing an ANP-led temporal artery biopsy service for patients with suspected giant cell arteritis


Abstract
Giant cell arteritis (GCA) is an uncommon autoimmune inflammatory vasculopathy that can lead to the destruction and occlusion of various arteries that consequently can cause serious complications such as stroke or sight loss. It is seen as a medical emergency. The most commonly affected vessel in GCA is the temporal artery in the side of the head, hence the condition is sometimes also referred to as ‘temporal arteritis’. This article discusses the introduction of an advanced nurse practitioner-led temporal artery biopsy service.
This article provides a summary of the symptoms, diagnosis, treatment and management of giant cell arteritis (GCA) in order to provide context for a review of the introduction of an advanced nurse practitioner (ANP)-led temporal artery biopsy service (TAB).
According to the National Institute for Health and Care Excellence (NICE) (2020), GCA is defined as an autoimmune chronic vasculitis which is associated with inflammation within the muscular walls of the arteries. The condition is sometimes also referred to as ‘temporal arteritis’ due to the temporal artery in the side of the head often being affected (Vasculitis UK, 2019) (Figure 1).
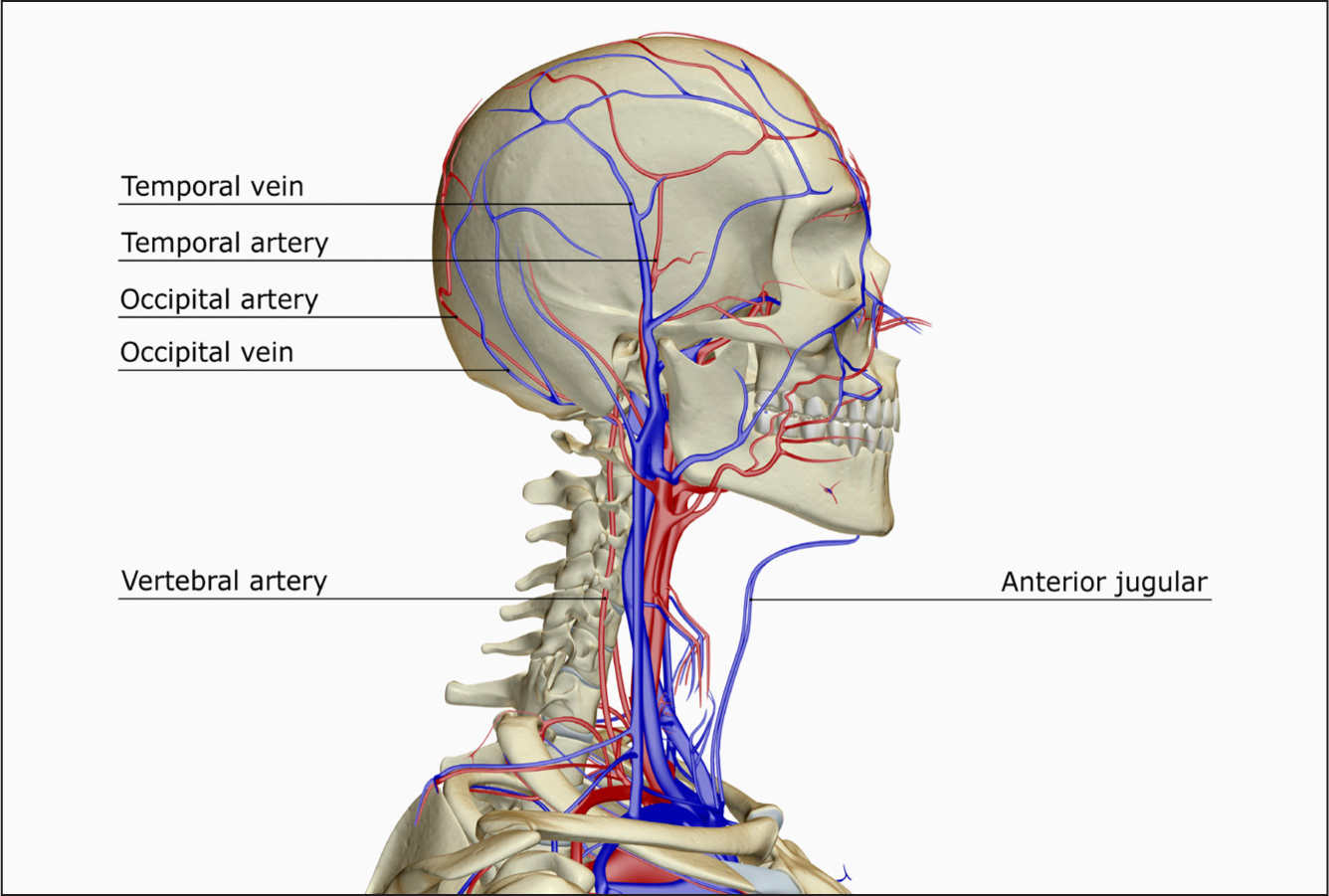 Figure 1. A lateral view of the blood supply of the head and neck, showing the position of the temporal artery
Figure 1. A lateral view of the blood supply of the head and neck, showing the position of the temporal artery
The cause of GCA is unknown, although genetic and environmental factors have been linked to a predisposition to the disease (Genetic and Rare Diseases Information Center (GARD), 2017). GCA is predominately associated with affecting the medium to large arteries in the head, especially extracranial branches of the carotid artery and the ophthalmic artery (NICE, 2020). Other arteries elsewhere in the body can also be involved, including, for example, the aorta, but this is uncommon within those diagnosed with GCA (National Institute of Arthritis and Musculoskeletal and Skin Diseases, 2016).
Register now to continue reading
Thank you for visiting British Journal of Nursing and reading some of our peer-reviewed resources for nurses. To read more, please register today. You’ll enjoy the following great benefits:
What's included
-
Limited access to clinical or professional articles
-
Unlimited access to the latest news, blogs and video content