

Psoriasis is a chronic, immune-mediated dermatological condition (Boehncke and Schön, 2015), affecting approximately 2% of the UK's population (NHS website, 2022a). The disorder typically presents as flaking skin patches that evolve into scales, exhibiting diverse appearances based on an individual's skin tone. Although psoriasis may cause minor irritation for some people, it can significantly impact others' quality of life, particularly those experiencing severe manifestations.
This article offers an analysis of psoriasis in the nursing context, encompassing risk factors, aetiology, pathophysiology, clinical classification, causative factors, triggers, diagnosis, treatment, and nursing considerations for patients living with the condition.
Risk factors and aetiology
Psoriasis is a complex disease with numerous risk factors and a multifactorial inheritance pattern. Approximately one-third of affected patients have a first-degree relative with the disorder, suggesting a hereditary predisposition (NHS website, 2022a). Genome-wide association studies have discovered several genetic loci related to psoriasis susceptibility; however, the exact mechanisms through which these genetic factors contribute to the condition's development remain to be elucidated (Rendon and Schäkel, 2019).
Environmental factors also significantly influence the onset and exacerbation of psoriasis. Stressful physiological and psychological events have been linked to the initiation and worsening of the disorder (National Psoriasis Foundation, 2022a). The Koebner phenomenon, in which new psoriatic lesions emerge at the site of skin injury, can trigger psoriasis due to direct skin trauma (NHS website, 2022a). Additionally, streptococcal throat infections may contribute to the development or exacerbation of psoriasis (NHS website, 2022a).
Human immunodeficiency virus (HIV) infection has not been identified as a direct trigger for psoriasis; however, it may exacerbate pre-existing disease (NHS website, 2022a). As HIV infection progresses and weakens the immune system, psoriasis frequently worsens (Gisondi et al, 2014). It is important to note that the relationship between HIV and psoriasis is complex, and further research is needed to elucidate the underlying mechanisms (Menon et al, 2010).
In addition to HIV, other risk factors and lifestyle factors have been associated with the development and exacerbation of psoriasis. Tobacco use has been shown to increase the risk of developing psoriasis and may worsen existing disease (Armstrong et al, 2013). There is a reported correlation between a higher BMI and an increased risk of psoriasis, with studies suggesting that weight loss can enhance symptom improvement (Naldi et al, 2008). Additionally, excessive alcohol consumption has been linked to an increased risk of developing psoriasis and may exacerbate the severity of the disease (Brenaut et al, 2013). Consequently, effective management of these risk factors, along with proper medical treatment, may help improve psoriasis symptoms and overall quality of life for affected individuals.
Pathophysiology and clinical classification
Psoriasis is an immune-mediated disease and many patients will have a genetic predisposition, but no distinct immunogen has been identified. The presence of cytokines, dendritic cells, and T lymphocytes in psoriatic lesions has prompted the development of biologic therapies (Rendon and Schäkel, 2019).
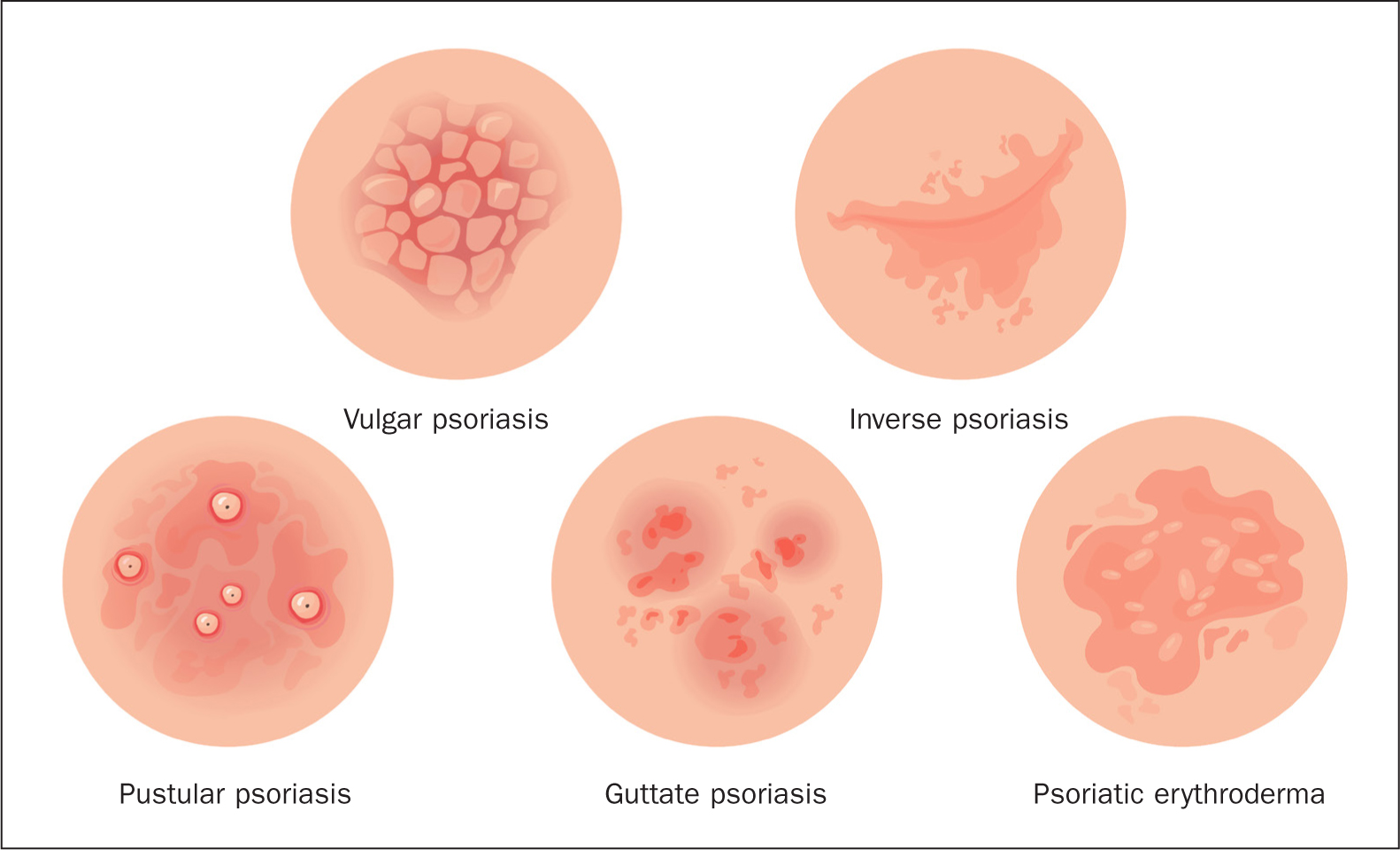
Dermatological manifestations of psoriasis are varied, with psoriasis vulgaris, also known as plaque-type psoriasis, being the most prevalent type (NHS website, 2022a). The terms psoriasis and psoriasis vulgaris are used interchangeably in the scientific literature. However, there are important distinctions among the different clinical subtypes, including inverse psoriasis, guttate psoriasis, pustular psoriasis, and erythrodermic psoriasis (Figure 1):
- Inverse psoriasis (also called intertriginous): is found in skin folds, such as in the armpits, groin and under the breasts (National Psoriasis Foundation, 2022b)
- Guttate psoriasis: appears as small, round spots called papules that are raised and sometimes scaly. Papules are caused by inflammation in the skin and often appear on the arms, legs, and torso (National Psoriasis Foundation, 2022c)
- Pustular psoriasis: symptoms include pustules (white or yellow, pus-filled, painful bumps) that may be surrounded by inflamed or reddened/discoloured skin (NHS website, 2022b)
- Erythrodermic psoriasis: this is a rare form of psoriasis that affects nearly all the skin on the body. This can cause intense itching or burning. Erythrodermic psoriasis can develop suddenly and may need emergency medical treatment (NHS website, 2022b).
Causes and triggers
Although the exact cause of psoriasis remains unknown, researchers have identified that the immune system and genetics play crucial roles (National Psoriasis Foundation, 2022a). The genetics of psoriasis are complex, and it is possible to develop the condition even without a family history of the disease. A triggering event may cause a change in the immune system, resulting in the onset of psoriasis symptoms. Common triggers for psoriasis include stress, illness (particularly streptococcal infections), injury to the skin, and certain medications (National Psoriasis Foundation, 2022a). Consequently, psoriasis triggers vary among individuals. What may exacerbate one person's psoriasis might not impact another. Common psoriasis triggers include stress, which is one of the most prevalent factors. Simultaneously, a psoriasis flare can cause stress, creating a seemingly endless cycle. However, relaxation techniques and stress management may help prevent stress from affecting psoriasis. Psoriasis can appear in areas of the skin that have been injured or harmed, a result of the Koebner phenomenon, where scratches, sunburn, bug bites, and vaccinations can all trigger psoriasis flares (NHS website, 2022a).
Diagnosis
A GP can often diagnose psoriasis based on the skin's appearance. In rare cases, a small skin sample, or biopsy, will be sent to a laboratory for examination under a microscope to determine the exact type of psoriasis and rule out other skin disorders such as seborrhoeic dermatitis, lichen planus, lichen simplex, and pityriasis rosea (NHS website, 2022a). Patients may be referred to a dermatologist, if the diagnosis is uncertain or if the condition is severe. If a doctor suspects psoriatic arthritis, a complication of psoriasis, the patient may be referred to a rheumatologist, a specialist in arthritis. Blood tests may be conducted to rule out other conditions, such as rheumatoid arthritis, and X-rays of the affected joints may be taken (NHS website, 2022a).
Treating psoriasis
Although there is no definitive cure for psoriasis, various treatments can alleviate symptoms and improve the appearance of affected skin. Treatment options for psoriasis range from topical therapies and phototherapy to systemic treatments, depending on the severity and extent of the disease (Armstrong et al, 2020).
Topical treatments
Most psoriasis patients will benefit from using an emollient, to reduce water loss, cover the skin with a protective film and help to reduce itching and scaling (NHS website, 2022a). For mild-to-moderate psoriasis, topical treatments are often the first line of therapy (Menter et al, 2019). These treatments are applied directly to the skin and include:
- Vitamin D analogues: (such as calcitriol) these are a synthetic form of vitamin D that help slow down the growth of skin cells and reduce inflammation (Lebwohl, 2002). They are available in various forms, including creams, ointments, and lotions
- Topical corticosteroids: these anti-inflammatory medications help reduce inflammation, itching, and redness associated with psoriasis. Examples include hydrocortisone, betamethasone, and clobetasol (Menter et al, 2019). It is important to note that long-term use of potent corticosteroids can lead to side effects such as skin thinning, so they should be used under the supervision of a health professional.
Phototherapy
Also known as light therapy, phototherapy is used to treat moderate-to-severe psoriasis when topical treatments have been ineffective or are insufficient (Menter et al, 2020). This treatment involves exposing the affected skin to specific types of ultraviolet (UV) light. Phototherapy options include:
- Narrowband UVB (NB-UVB) therapy: This is the most common form of phototherapy for psoriasis, involving exposure to a narrow range of UVB light wavelengths (311-313 nm – 1 millionth of a millimetre) (Menter et al, 2019). It helps slow down the growth of skin cells and reduces inflammation
- Psoralen plus UVA (PUVA) therapy: this treatment combines the oral or topical administration of a photosensitising agent called psoralen with exposure to UVA light. PUVA therapy is typically reserved for more severe cases or when NB-UVB is ineffective (Menter et al, 2019).
Systemic treatments
Systemic treatments are used for severe psoriasis or when other treatments have failed. These medications work throughout the entire body and include:
- Oral medications: methotrexate, acitretin, and ciclosporine are examples of oral medications prescribed for psoriasis. These drugs suppress the immune system or reduce the rate of skin cell growth (Menter et al, 2019)
- Injectable biologic agents: biologics are a class of medications derived from living organisms that target specific components of the immune system. Examples include tumour necrosis factor (TNF) inhibitors, such as adalimumab, etanercept, and infliximab, and interleukin inhibitors, such as ustekinumab, secukinumab, and ixekizumab (Armstrong et al, 2020).
Nursing considerations for people living with psoriasis
Although psoriasis may be a minor irritation for some, it can significantly impact the quality of life for those more severely affected (NHS website, 2022a). For example, individuals with psoriasis may experience low self-esteem due to the condition's effect on their appearance. It is also common for patients to develop tenderness, pain and swelling in the joints and connective tissue, a condition known as psoriatic arthritis (NHS website, 2022a). Nurses play a crucial role in providing comprehensive care, including education, emotional support and assistance in managing symptoms and treatment side effects.
Clinical guidance for nursing practice
The National Institute for Health and Care Excellence (NICE) clinical guideline CG153 on Psoriasis: Assessment and Management (NICE, 2017) provides key information that nurses need to know to provide comprehensive care for individuals with psoriasis. Table 1 sets out the essential recommendations for nurses. By following the NICE clinical guideline, nurses can provide evidence-based, comprehensive care for patients with psoriasis, improving their overall wellbeing and quality of life.
Table 1. Summary of NICE recommendations for nursing people with psoriasis
| Assessment | Nurses should assess the severity of psoriasis, its impact on a patient's physical, psychological, and social wellbeing, and the presence of any relevant comorbidities. They should use validated tools, such as the Psoriasis Area and Severity Index (PASI) and the Dermatology Life Quality Index (DLQI), to assess the severity of the disease and its impact on the patient's quality of life |
| Patient education and support | Nurses should provide information about psoriasis, its management, and available treatment options. They should discuss the potential benefits and risks of treatments and support patients in making informed decisions. Nurses should also provide advice on self-care, trigger avoidance, and appropriate use of emollients and other topical treatments |
| Treatment options | Nurses should be familiar with various treatment options for psoriasis, including topical treatments (such as corticosteroids, vitamin D analogues, and combination therapies), phototherapy, and systemic therapies (such as methotrexate, ciclosporin, and biologic agents). They should collaborate with other health professionals to develop individualised treatment plans for patients based on the severity of the disease, the patient's preferences, and the potential risks and benefits of each treatment option |
| Monitoring and follow-up | Nurses should monitor patients' response to treatments, assess for potential side effects, and ensure adherence to treatment plans. They should also provide regular follow-up and adjust treatment plans as needed, based on the patient's response and any changes in their clinical condition |
| Comorbidities and complications | Nurses should be aware of potential comorbidities associated with psoriasis, such as cardiovascular disease, metabolic syndrome, and mental health issues. They should collaborate with other health professionals to address these comorbidities, provide appropriate referrals, and ensure comprehensive patient care |
| Psoriatic arthritis | Nurses should be vigilant for signs and symptoms of psoriatic arthritis, a common complication of psoriasis. They should collaborate with rheumatologists and other health professionals to manage this condition effectively |
Conclusion
Psoriasis is a complex, chronic skin condition that poses unique challenges for patients and healthcare providers alike. Nurses play a critical role in supporting individuals living with psoriasis, helping them manage their symptoms, understand their triggers, and navigate the complexities of treatment options. By staying informed on the latest research and recommendations, nurses can ensure they provide the best possible care for their patients living with psoriasis.
Key Points
- Psoriasis, an incurable skin condition, has various treatment methods to manage symptoms, ranging from topical therapies and phototherapy to systemic treatments based on disease severity
- Topical treatments such as vitamin D analogues and corticosteroids can slow skin cell growth and reduce inflammation, while phototherapy involves UV light exposure to treat moderate-to-severe psoriasis
- Systemic treatments, including oral medications and injectable biologic agents, work throughout the entire body and are used for severe psoriasis
- Psoriasis can significantly impact the quality of life of severely affected individuals, necessitating careful nursing considerations