
The emergency department (ED) is often the first stop for people in need of immediate healthcare attention, including those with injuries related to self-harm. Self-harm has been acknowledged as a public health concern, both nationally and internationally (Murray et al, 2013). It requires a continuous review of the evidence base and innovation in practice.
This article examines the perceived negative attitudes of healthcare staff towards people who self-harm and discusses how to address these. The recently commissioned National Institute for Health Research project, which will investigate how to support and protect those who self-harm, led by Professor Rose McCabe at City, University of London (Quadir, 2019), is a good example of how self-harm and patient experience is high on the Government's healthcare agenda, especially in relation to exploring the evidence base to support service improvement.
This article draws on the literature to identify and highlight how perceived negative attitudes from healthcare staff regarding self-harm presentations can be addressed in EDs. A clear gap in research and education in relation to staff knowledge has been noted by the National Institute for Health and Care Excellence (NICE) (2018). An initial exploration of self-harm aetiology and causes will address the knowledge gap described by NICE (2018). This will set the scene for exploring the resulting negative attitudes held by healthcare staff, which are informed by common myths.
The author has experience of working in an ED in a psychiatric liaison team (PLT) nurse role, and this article is influenced by nursing experiences and the desire to influence change and service development. The negative staff attitudes highlighted in this article are primarily informed by the author's experiences and supported by evidence from the literature.
What is self-harm?
Self-harm is a deliberately caused injury or poisoning, usually viewed regardless of stimulus, which may or may not include suicidal intent (Hawton et al, 2003; Clements et al, 2016; NICE, 2018). It has been interpreted as a maladaptive reaction to acute emotional anguish and a means of self-preservation and emotional regulation. Self-harm is not a mental illness in its own right but a symptom of underlying emotional distress triggered by any number of personal reasons.
The term ‘self-harm’ used in the UK is synonymous with the discouraged term ‘deliberate self-harm’, which has negative connotations related to the word ‘deliberate’; however, the ICD-11 (World Health Organization, 2019) uses the similarly negative prefix ‘intentional’.
Prevalence
Routinely collected ED data on self-harm presentations in England, both locally and nationally, indicate the scale and demand exerted by self-harm incidence on health services, particularly EDs. Notably, the bulk of this data is local and is not representative of all hospitals in England or the UK as a whole.
A multicentre study covering Oxford, Manchester and Derby found there was a total of 13 547 self-harm episodes recorded between 2010 and 2012 (Clements et al, 2016). The same study found that Hospital Episode Statistics (HES) ED data suggested there were 9600 yearly episodes, while HES admission data gave a total annual figure of 8096 (http://www.hscic.gov.uk/hes) (Clements et al, 2016). In comparison, a previous study by Hawton et al (2007) noted there were 220 000 annual cases of self-harm ED presentations across England. The Department of Health (DH) (2017) and Rayner et al (2019) noted that numbers are continuing to rise, with England having the highest self-harm incidence rates in Europe. Notably, the interpretation and use of these statistics are complicated by the knowledge that people who self-harm do not all present to services. Regardless of this flaw, the statistics, though gathered locally, reflect the scale of demand on services.
Suggestions that the statistics highlight a consistent underestimation of 60% are a cause for concern when it comes to estimating potential demand for services (Clements et al, 2016). The reality is that more than half of patients who self-harm do not present to services. The figures for estimated demand for services therefore do not show an accurate picture of how services meet the needs of this population.
There is clear need for a systematic review of the current evidence base and service provision to investigate reasons why 60% of people who self-harm are not accessing services (Clements et al, 2016). A uniform, national method of collecting data related to self-harm presentations would ease the process of interpretation and aid service planning. The above statistics, although helpful in terms of determining increases in incidence, are difficult to synthesise because of variations in data collection methods and points of collection. In this instance, there was marked variation between presenting and admission cases because some hospitals record presentation and others admission. The HES identified only hospital presentations that clearly showed self-harm as the initial presenting complaint (Singhal et al, 2014). Coding may be complicated by the aetiology of self-harm being compounded by other complexities related to the coding of self-harm incidence in ED; for example, people who self-harm may present to ED with different complaints, such as stomach pains after an overdose.
In response to public health concerns informed by prevalence and demand on services, NHS England devised Commissioning for Quality and Innovation (CQUIN) quality improvement indicators for 2017–2018 and 2018–2019 in an attempt to reduce ED attendance for predominantly mental health problems (NHS England, 2018). A particular focus was given to ‘frequent attenders’, who account for 10% of self-harm ED attendances (Ness et al, 2016). The literature suggests that 20% of patients who self-harm have yearly repeat presentations, while 10% present again within 10 days of ED discharge (Bergen et al, 2010). The latter population is categorised as high risk in that they experience double mortality rates with related service demand and health cost implications (Moe et al, 2016). The CQUIN targets were designed to increase the focus on this population group by improving standards of care, treatment and risk management. NICE (2018) has updated and implemented best practice guidelines, which are intended to foster and enforce seamless service provision by providing a clear outline of outcomes, overarching indicators and improvement areas in relation to self-harm (NICE, 2018). Theoretically, the use of CQUIN targets should streamline processes and decrease the number of ED presentations. The CQUIN targets' attention to frequent attenders appears to be economically driven, with the aim of easing pressure on services. They appear to neglect the fundamental reasons why people who self-harm present at EDs in the first place, which is to seek support in addressing underlying distress. Although the NICE guidelines (2018) provide a safe framework to deliver care and staff education, addressing negative staff attitudes in relation to self-harm should also be prioritised.
As triage nurses are the first point of contact in the ED, it is imperative they are encouraged not only to gain skills in assessing and managing risk to deal with increased presentations, but also to do so in a manner that demonstrates compassion and person-centred care, focusing on reducing emotional distress.
Self-harm and suicide
Presenting with self-harm or having self-harm ideation does not necessarily mean a patient had or has suicidal intent (Tørmoen et al, 2013). Motives can vary, and depend on the reasons for triggering and perpetuating the act. Self-harm and suicidal ideation can be evident in the same presentation.
Clinicians need to be able to explore and understand the relationship between suicide and self-harm and its links with mortality risk. Self-harm is a contributory—and the strongest—risk factor for completed suicide and premature death (Hawton et al, 2015; Healthcare Quality Improvement Partnership, 2017). The national suicide prevention strategy in England (DH, 2017) noted that 68% of people who die by suicide had previously self-harmed. Links with a high mortality risk further demonstrates that self-harm as a public health concern.
Self-harm methods
An epidemiological study assessing self-harm trends specified that the most common forms of self-harm are the use of medication and cutting, with 75% of the self-harm population presenting because of self-poisoning (Geulayov et al, 2016). Other methods may include ingesting objects or toxic substances, burning or scalding the skin with cigarettes or strong acids, banging of various body parts, pulling out hair in clumps or gradually, and excessive substance use. This list is not exhaustive. Methods of self-harm vary and clinicians should not make assumptions around suicidal motivation based on method used (Dhingra and Ali, 2016).
Understanding causes
It is imperative for clinicians to ascertain the reasons for self-harm on each presentation. Self-harm must be taken seriously on every occasion, irrespective of the reasons behind the act, frequency of presentations or severity.
The majority of people who self-harm have a mental illness, most commonly depression, borderline personality disorder/emotionally unstable personality disorder (EUPD), bipolar disorder, drug and alcohol use disorders, and can be linked to trauma (Hawton et al, 2013). Self-harm is a diagnostic criterion for borderline personality disorder/EUPD and can also be seen in patients with psychosis and schizophrenia (Singhal et al, 2014).
Understanding the triggers and thoughts related to self-harm can inform assessment and treatment options. Triggers for self-harm may include (Singhal et al, 2014; Dhingra and Ali, 2016):
Self-harm cycle
Although heterogeneous, the patterns of self-harm are primarily similar and can follow the cycle illustrated (Figure 1), which has been adapted from Brain et al (1998). If staff understand the psychophysiology cycle of self-harm, this will assist in identifying potential distress and related feelings.
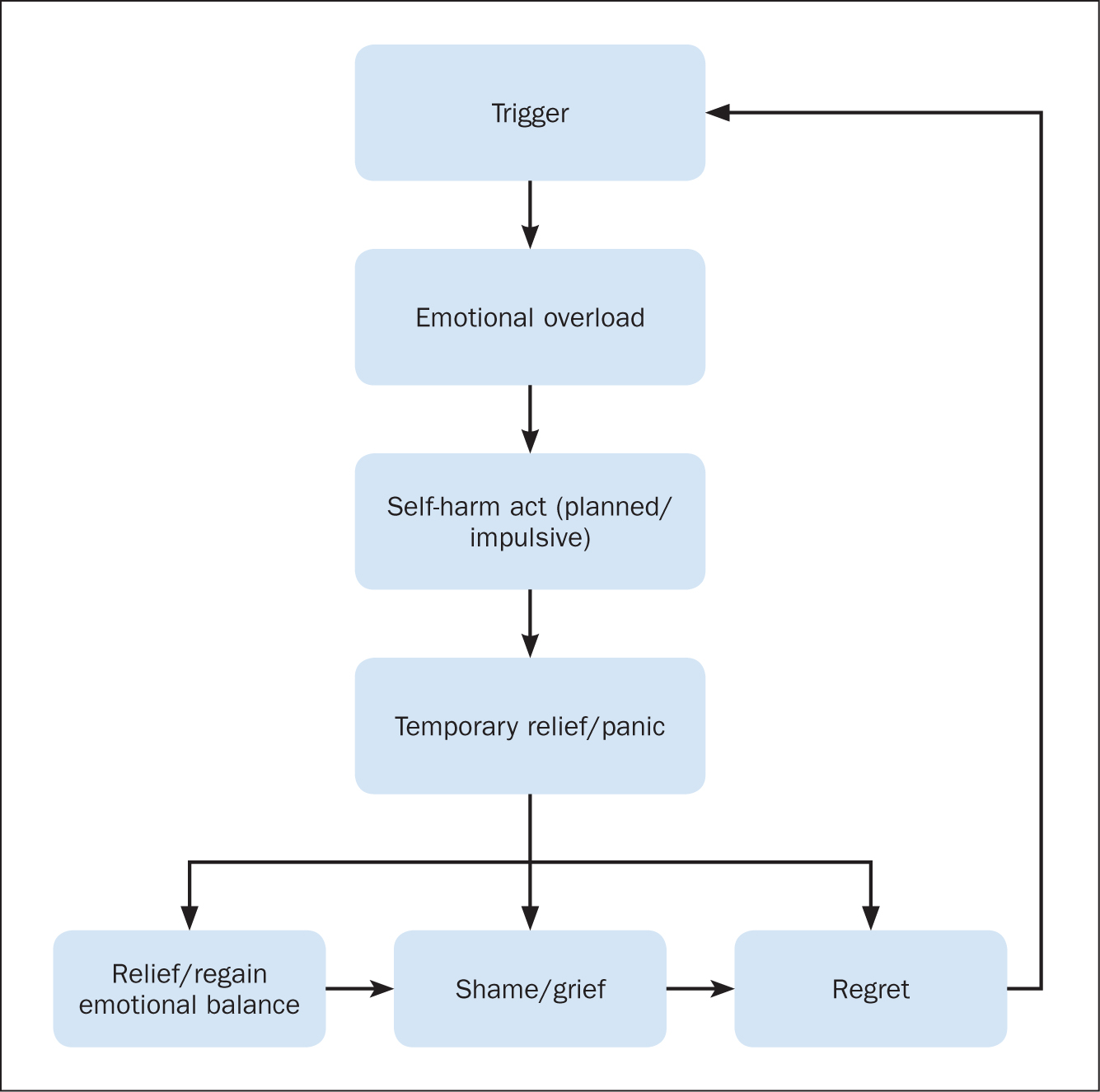
Clinicians must comprehend the fluid nature of self-harm thoughts and be aware that, by the time a patient presents at the ED, their thoughts and feelings might be anywhere on the psychophysiology cycle in Figure 1. Klineberg et al (2013) highlighted the subjective nature of self-harm thoughts; although the Brain et al (1998) cycle may represent a typical psychophysiology cycle, there is little evidence to suggest that all the stages apply in every case. It is imperative to keep in mind that the sequence of feelings may not be linear.
The fluid nature of a patient's emotions following self-harm further explain the self-harm cycle. In relation to self-harm serving the purpose of relieving emotional distress, momentary relief may be experienced. However, relief is temporary if underlying primary triggers persist. In addition to the intense emotions that would have initially driven the self-harm act, the patient is likely to experience strong feelings of guilt, shame and regret. These feelings may increase emotional vulnerability, leading to increased sensitivity, especially in relation to attitudes from staff and significant others (Rayner et al, 2005). These feelings, together with external stimuli, might either perpetuate the cycle or deter the person from further self-harm. This is a period where some patients benefit from feeling temporary relief. Experience of the sought-after temporary relief may lead to the patient using self-harm as a future maladaptive coping mechanism, a means of self-preservation and emotional regulation in the event of subsequent emotional distress.
Some authors have discussed the addictive qualities of self-harm, especially in repeat acts, as a maladaptive coping mechanism (Mangnall and Yurkovich, 2008). Use of self-harm as a maladaptive coping mechanism leads to entrenched difficulties in regulating emotions. Therefore, in relation to ED, it is key for triage clinicians, as the first point of contact, to understand the cycle of emotions and encourage patients to engage with services and explore alternative ways of managing their emotions.
Rayner et al (2005), in an attempt to explore the cognitive emotional and behavioural effects of self-harm acts on professionals, created a theory to demonstrate how emotional responses can affect thinking processes (Figure 2). Professionals need to understand how negative attitudes, which may be driven by emotional reactions or a lack of knowledge, can result in negative countertransference, where a patient feels worthless because they perceive that this is how professionals view them. This can perpetuate the self-harm cycle.
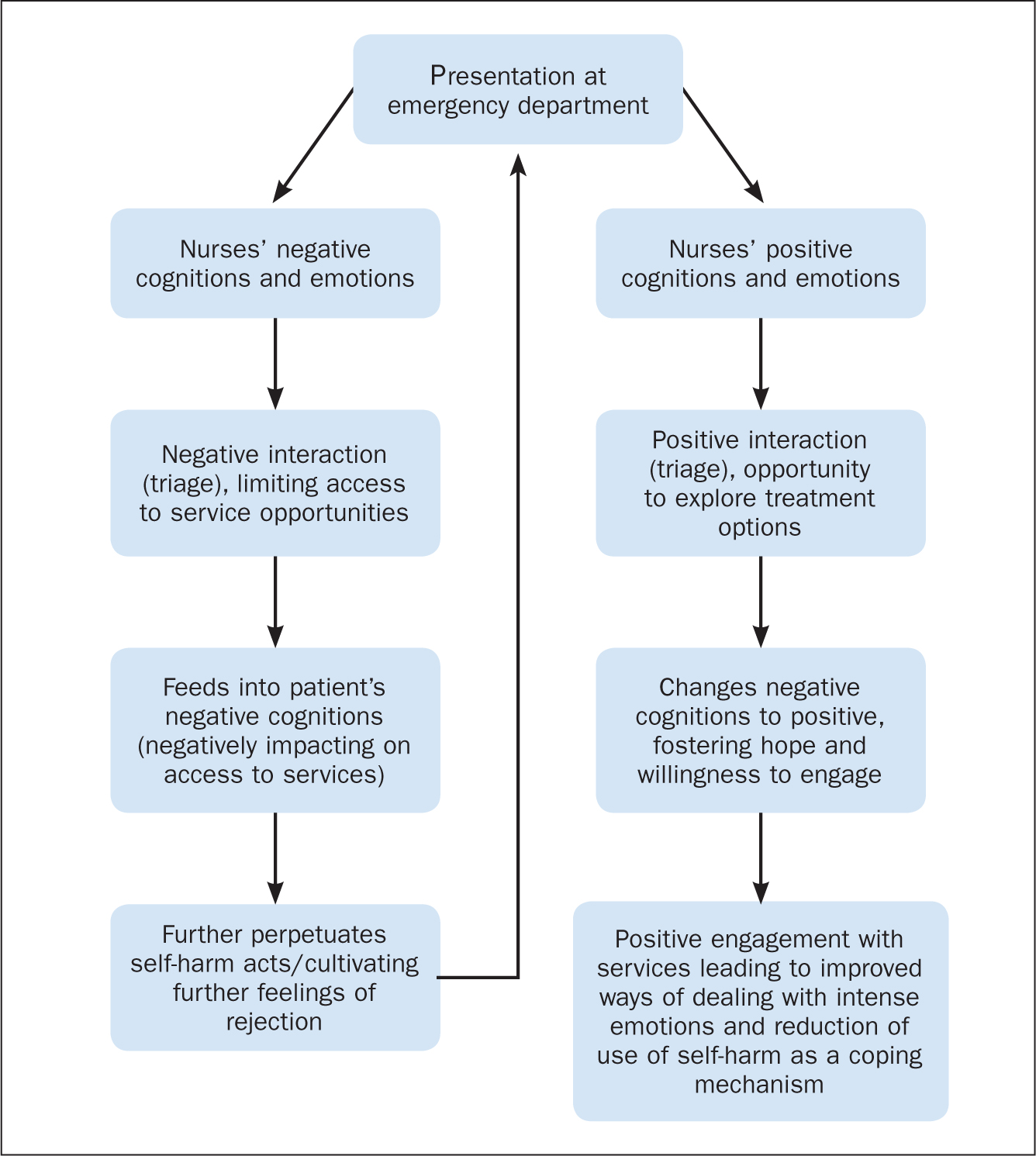
The adapted Rayner et al (2005) cycle can be used in supervision to address the stages using the CARE (containment, awareness, resilience and engagement) framework (McAllister and Walsh, 2003). This reflection tool is designed to help the nurse identify the intervention stages related to caring for people who present having self-harmed. Figure 2 illustrates what might hinder the intervention stages. Understanding the Brain et al (1998) cycle and using the adapted Rayner et al (2005) cycle and the CARE framework will help nurses to understand self-harm and aid reflection.
Self-harm and emergency department presentations
Evidence suggests that people who self-harm may not present to an ED for numerous reasons. Horrocks et al, (2002; 2005) and McDougall and Brophy (2006) postulated that a hostile ED reception because of negative staff attitudes can be a deterrent and perpetuate negative feelings, and discourage people from accessing services. Hence attending an ED can be a distressing experience for some people who self-harm (Royal College of Psychiatrists, 2010; Rayner et al, 2019). People may also not present to EDs because they may be secretive as self-harm is a private act. This may be driven by social stigma around self-harm behaviour or the feelings of shame and regret discussed before (Brain et al 1998; Lancet, 2012; Gibson et al, 2019).
Negative attitudes from professionals towards people who self-harm can have a profound impact on recovery, as the Rayner et al (2005) adapted cycle illustrates. Some studies have observed that clinicians' negative attitudes can potentially unravel good practice that influences recovery (Simpson, 2006). Such negative attitudes may be driven by staff having a limited understanding of the reasons for self-harm and treatment outcomes, as NICE (2018) acknowledges. It is recognised that offering high-quality assessment and treatment and reducing distress in a demanding ED environment can be a challenge. However, acknowledging patients' experiences and addressing the possible impact of negative staff attitudes directed at people who self-harm when attending an ED is key to improving treatment outcomes. With figures suggesting a high incidence of self-harm, increasing demand for services and a large percentage of people who self-harm not presenting at ED or leaving without support, using patient experience to inform access to services should be paramount and steps should be taken to improve this situation.
It is important to explore not just the need for a biopsychosocial assessment and treatment guidelines, but the crucial nature of the contact at ‘stage 2: triage’ of the NICE Managing Self-harm in Emergency Departments flow chart (NICE, 2018).
Triage, as highlighted by NICE (2018), is a crucial point of ED contact. This is a juncture where most patients experience positive or negative attitudes around self-harm (Koning et al, 2018). To improve the quality of service provision related to negative staff attitudes, this article explores common myths and attitudes of clinicians that may be evident during the triage stage, and thereby hinder access to services.
Retributory or disparaging staff attitudes can be distressing for people who self-harm and may trigger further self-harm episodes or complete avoidance of services (Rayner et al, 2005). Raising self-harm awareness and recognition of how a positive user experience can be hindered by staff negative attitudes will have a positive impact on care and, potentially, improve outcomes. Negative attitudes driven by a lack of understanding of self-harm aetiology can impede access and success of subsequent psychosocial assessment, which can markedly reduce incidence of future self-harm (Healthcare Safety Investigation Branch (HSIB), 2018). Triage is the first contact with treatment services. It is pivotal in access to care and its crucial role should never be underestimated.
Negative attitudes to self-harm
The compounding factors relating to self-harm aetiology and treatment outcomes are contentious and this is acknowledged in the literature (Mangnall and Yurkovich, 2008). The ongoing debate highlighting that self-harm is not attributable to one single cause appears to perpetuate negative attitudes and contributes to further bias and stigmatisation. Clinicians' negative attitudes result in deleterious behaviours reinforced by dogma relating to their own belief systems and interpretation of self-harm. Unfortunately, negative attitudes impede information processing by both practitioner and patient and, in most cases, hinder access to services, leading to a revolving door of regular presentations at the ED (Maio and Haddock, 2010).
Saunders et al (2012) stated that negative staff attitudes were known to be prevalent in EDs compared with other clinical settings. However, attitudes can permeate all clinical areas. Professionals who are not based at EDs can display equally negative responses to people who self-harm. Negativity may be in response to burnout and overexposure to repeated incidents of self-harm.
Rayner et al (2019) examined the wide range of evidence that explored staff attitudes, especially in relation to repeated exposure to self-harm incidents, and made recommendations related to further education. Negative attitudes, especially when people present at ED, have been shown to perpetuate negative feelings (Horrocks et al, 2005), leading to patients perceiving that they are an encumbrance, which in turn compounds negative emotions and increases feelings of isolation. Similarly, medical staff with little understanding of the aetiology of self-harm might experience distress, anger and frustration, especially when treating patients who present regularly after self-harming (Richardson, 2004). The awareness of effects of implicit bias might help overcome prejudice and improve decision-making.
In addition, clinicians need to be able to reflect on their practice using the Rayner et al (2005) cycle. This will help them work towards improving their awareness of the impact of prejudice and stereotypes when assessing people who self-harm (FitzGerald and Hurst, 2017).
While experiencing mental ill health is associated with stigma, self-harm attracts greater stigma. A recent study by Gibson et al (2019) explored the stigma that student nurses associated with people who self-harm. The study aim was to develop and test an educational intervention to address this. This included examples of well-known celebrities who had mental health problems and who had self-harmed in exploring attitudes. After receiving the educational intervention, the student nurses demonstrated an increase in positive attitudes towards those who presented with self-harming behaviour, and a reduction in negative attitudes compared with their attitudes before they took part in the intervention.
In practice, the use of negative labels such as ‘frequent flyer’, even in treatment documents, continues to build barriers in terms of accessing treatment, which can further ostracise patients. Awareness of stigma and its implications should inform how nurses conduct assessments. It is imperative to give people who self-harm the opportunity to express how they feel in a safe environment, taking into consideration a growing evidence base that suggests that self-harm acts are largely triggered by past trauma and presenting patients may require psychological support as they may be reliving the traumatic incident (Gurung, 2018). Health professionals need to understand the stigma and its links to trauma if they are to offer compassionate treatment, devoid of prejudice. Stigma and related negative attitudes perpetuate common myths related to self-harm and these are unhelpful when accessing care.
Common myths
There are several common beliefs related to self-harm. The following list draws on work by Mangnall and Yurkovich (2008)Emerson (2010) and the author's personal observations and experiences of working in an ED:
Recommendations for practice
Psychiatric care in EDs
This article has acknowledged that following increased awareness of prevalence and mortality risks related to self-harm, there have been notable changes in practice, both nationally and locally driven. The integration of psychiatric liaison teams (PLTs) into ED departments has been a significant first step in improving access to services (NHS England and NICE, 2016). However, the purpose and function of PLTs needs to be extended beyond the role of assessment and be transformed to a structured, knowledge resource link in the ED, fostering a culture of evidence-based shared learning.
Training
Regular training for ED staff is crucial in terms of building a knowledge base addressing mental health stigma and negative staff attitudes, especially in relation to self-harm (NHS England and NICE, 2016; Rayner et al, 2019). PLTs should not be used only to provide ad hoc training and efforts should be made between ED and PLT staff to design an evidence-based, regular teaching programme, targeting underlying negative attitudes and skills deficits. This should not be the role of senior PLT staff only—all PLT team members should adopt an active role and this should be part of their job description. To date, there has been no evidence to suggest that PLTs provide regular structured training other than ad hoc training when they are assessing patients, yet education has been identified as key in addressing the knowledge gap that can address the presence of negative attitudes towards people who self-harm. Therefore, creating an evidence-based teaching schedule delivered by the PLT should be a priority.
An evidence-based programme will have the potential to harness the concerns cited in contemporary literature as it emerges and to develop and strengthen knowledge within teams. PLT teaching sessions should be incorporated in a structured induction and mandatory training and also be flexible enough to address emerging findings. There should be a focus on understanding, among other topics, the aetiology of self-harm, the nature and impact of implicit bias, the impact of implicit bias on assessment, treatment pathways and any other psychiatric concerns identified by research and systematic data collection.
A similar CPD programme that can be carried out in house is Connecting with People's training modules on Emotional Resilience, Self Harm Reduction, and Suicide Awareness (http://www.connectingwithpeople.org). The aim of this is not just to improve skills and attitudes of staff but also to foster a compassionate and dignified approach to assessing presenting patients in a hectic ED environment, with a move away from using statistics to measure success. This would promote a safe triage that should not only reduce distress but also bolster structured, evidence-based partnership working that can be replicated internationally.
Future consideration may be for PLT staff to extend such training to GPs in line with fully integrated community-based health care highlighted in the NHS Long Term Plan (NHS England and NHS Improvement, 2019). Well-articulated training and guidance would foster an environment where outcomes are measurable by use of regular structured service user feedback.
Guidance
Patients who self-harm and present at ED should be assessed using evidence-based assessment tools. EDs, following recommendations by NICE (2018), have implemented this practice in various forms nationally. Emergency care assessment documentation now has prompts in line with the National Confidential Enquiry into Patient Outcome and Death's (2017)Treat as One document, which promotes a cross-departmental strategy. Although there are variations noted by the Mental Health Crisis Care Concordat (DH, 2014), the active use of such documents demonstrates an increased level of priority and positive strides towards promoting integrated care. To date, any evidence base supporting the efficacy and use of such documents is scarce.
HSIB (2018) suggested there is a gap in service provision related to the lack of structured joint training for ED staff in using these documents. The HSIB (2018) report Investigation into the Provision of Mental Health Care to Patients Presenting at the Emergency Department has highlighted gaps and inconsistencies in care in EDs. It has identified variations between guidance from different national bodies in relation to initial assessment as an issue, impacting on consistency and quality measurement. The HSIB (2018) report urgently calls for a review of guidance related to the management of self-harm in EDs. The absence of a uniform, evidence-based assessment framework and guidance could make it difficult to address complex problems. The above-identified PLT training schedule could provide guidance when such gaps in knowledge become evident.
Professional integration
In a move to further integrate services, PLT nurses with additional training in physical care should be rotated into the ED triage team. This will strengthen partnership working and reflect the Nursing and Midwifery Council (NMC) (2018) standards for education. The NMC standards mandate that all new nursing registrants should practise at an advanced level from the time they enter the register, to take a modern, innovative approach to service provision (NMC, 2018). The NMC guidelines recommend including plans to give students experiences and understanding of all four fields of nursing in the curriculum before registration.
It is expected that all future nurses will be confident in offering assessment and care in increasingly complex environments. Bringing PLT nurses into the triage environment will not only be in line with the NMC standards but will also improve patients' access to care, make mental health education more accessible to ED nurses and directly influence improvements in screening and identification of future training needs.
Care planning
Regular joint governance meetings between EDs and PLTs would ensure effective formulation and management of ED joint care plans designed to provide consistent care for self-harm frequent attenders who have complex, long-term needs (Hockey et al, 2014). Evidence supporting the efficacy of care plans in reducing frequent attendance is yet to identify improved health outcomes. Currently, these care plans appear to focus on ‘risk management’ rather than on improving care (Peddie et al, 2011).
Patients should be involved in the formulation of care plans and it is essential that they are invited to scheduled reviews. Although care plans formulated after strategic meetings are shared with EDs, the level of patient involvement is unclear and there is no shared schedule between EDs, PLTs and any other mental health teams to suggest how often the care plans need to be reviewed. There is limited guidance in relation to when these care plans need to be updated, especially if a patient is not being managed under the care programme approach.
Further research is vital to identify the use and efficacy of care plans for frequent attenders (Smith and Chambers, 2017). Failure to manage the formulation, implementation and review of these care plans may negatively affect treatment outcomes, leading to an increase in self-harm episodes and possibly death.
With no systematic approach to implementation of care plans involving mental health services, it is unclear what the views of staff are, especially in relation to such care plans being used for people who regularly self-harm. Further research is required on the purpose and use of such joint documentation.
Frustration of treatment refusal
Given the complex nature of self-harm, clinicians need to avoid the ‘all or nothing’ approach. There may be times when patients who self-harm refuse treatment (Jacob et al, 2005). This may conflict with reasons for presenting at ED in the first place. Refusal of treatment does not justify withholding information that might help the patient manage self-harm in the future, although clinicians might do this in frustration. Regular training would address this in the process of exploring implicit bias.
Conclusion
Considering these recommendations in practice will not only address negative attitudes, increase the knowledge base and promote an integrated approach but also improve the overall patient experience. It will provide an opportunity to ensure continuous monitoring and address barriers to care, including staff attitudes, by the pursuit and use of evidence-based practice. This will ensure a move towards joined-up care, as suggested by the NHS Long Term Plan (NHS England and NHS Improvement, 2019).
Further research investigating staff negative attitudes and experiences would better inform how negative attitudes develop and permeate systems in care. It will inform pathways to address such attitudes and map ways of embedding this in policy.